Medical/Patient Care
Questions pertaining to medical or patient care
What are the recommendations/contraindications for concurrent HBO and Chemotherapy/Radiation?
This answer is from the recognized physician expert in the field of hyperbaric medicine dealing with oncological disease – John Feldmeier, DO.
“There is no easy answer to this question. We still struggle to answer the question of whether patients with a remote history can have HBO2.
Although I believe that in almost all cases this would be safe. There is very little published data with concurrent therapy. The issue of concurrent chemo/ HBO2 has next to no published information and really has become a fairly recent issue because patients are now living longer with active malignancy. There are more and more options for systemic treatment and quality of life issues are pertinent for patients even when they have active disease. The scenario where this becomes an issue is when a patient has had prior radiation, has a complication, needs HBO2 but is receiving chemo probably because recurrent or residual cancer has been found.
Chemo comes in many varieties with traditional cytotoxic drugs in at least 8 categories and now with more options including immune therapies and anti-angiogenic therapies. It is impossible to make a universal recommendation applicable to all chemotherapies.
Some of these drugs mediate their anti-tumor response through free radicals which cause chemical bond breaks in the DNA leading to reproductive death. Some are antibiotics: some are spindle cell blockers etc., etc. Those that mediate cytotoxicity through free radicals are likely to have their effect enhanced in the tumor and normal tissues.
This was the basis of using HBO2 as a sensitizer to radiation done from late 50's to early 70's. Since the therapeutic goal is to enhance QOL, this would not be perceived as an appropriate effect.
As I am sure, most of you know Eric Kindwall's book declares there to be a contraindication to Adriamycin and Cisplatin. This precaution is based on pretty weak evidence. On the other hand Dick Clarke has done a preliminary study with colleagues at U of Chicago using HBO2 along with Cisplatin and radiation without signs of increased toxicity.
I am especially concerned about Bleomycin and Avastin. Jake Freiberger, MD of Duke U. has reviewed their experience in treating patients with a PAST not concurrent history of Bleomycin exposure without a demonstrable ill effect. I would not give Bleo concurrently with HBO2. Avastin and some of the other so called biologics (Erbitux) target growth factors including VEGF to exert their effect. Since we enhance VEGF with HBO2 are we diminishing the anti-cancer effects of Avastin? Will HBO2 be effective if VEGF is being suppressed by the Avastin? We don't know.
My operational recommendation is: 1)to avoid chemo and HBO concurrently whenever possible.2) If you do give concurrently wait a few half-lives perhaps 4 or 5 to see serum levels significantly lowered before resuming HBO2 after each chemo administration. Half-lives for all the drugs are published. Avastin is 60 days!! 3) I would avoid Avastin and some of the other biologics as well as Bleomycin as concurrent therapies.“
I wanted to ask whether you had any knowledge of clinical circumstances or literature regarding having a patient with a 20+ year old mechanical aortic valve undergo HBO2. The valve has not been pressure tested by the manufacturer?
There are no pressure-sensitive components in a mechanical valve, since it contains no gas pockets. There are no issues with respect to hyperbaric oxygen therapy regarding a prosthetic valve.
My understanding is that air breaks are uncommon anymore in the HBO2 community and I understand that there is a greater risk of O2 toxicity @ 2.4 ATA or greater. Is there any documented evidence for the need of air breaks during the hyperbaric treatments?
Thank you for your question. The UHMS HBO2 safety committee can provide information to assist you in answering your question, but the ultimate responsibility for these types of questions rests with the medical director and safety director of your facility.
The SC cannot recommend medical practice. The hyperbaric treatment protocol is the responsibility of the medical director and the safety director.
Air breaks are used in the clinical setting for two primary reasons. The first to reduce oxygen toxicity involving the central nervous system. The second is to reduce oxygen toxicity to the pulmonary system. Due to the complexity of our patients and the underlying disease processes, the patient may present with conditions that could possibly lead to a lower threshold limit for oxygen toxicity (i.e. fever, low blood sugars, medications).
A review conducted in 2003 by Hampson & Atik demonstrated an overall seizure rate of 1 in 3,388 treatments or 0.03% (Hampson & Atik, 2003). In 2011 Banham examined the incidence of oxygen toxicity seizures over 41,273 treatments for 3,737 patients and found the overall rate was 0.06% or 6/10,000 exposures with a higher incident rate in patients treated at increased pressures (0.56% at Navy Treatment Table 6 for dysbarism) (Banham, 2011). Another article reported zero per 10,000 at 2.0 ATA, 15 per 10,000 at 2.4/2.5 ATA and 51 per 10,000 at 2.8 ATA (Heyboer et al. 2014). Patients treated for CO poisoning or decompression illness have an incidence as high as 0.5-2%, presumably due to a combination of CNS injury and higher PO2 (2.8-3 ATA) used for treatment of those conditions (Hampson et. al. 1996; Banham, 2011). A 2016 retrospective chart review of 2334 patients treated at a hyperbaric center in Israel found a seizure incident rate of 0.3% (7 patients); however, they determined “only one patient (0.04%) had a true oxygen toxicity event” (Hadanny et al. 2016).
Major pulmonary oxygen toxicity has not been reported during routine clinical hyperbaric treatment, although there is a theoretical risk in patients who receive oxygen within a short interval after certain chemotherapeutic agents such as bleomycin and mitomycin C.
The rationale for air breaks is based upon a study in which volunteers breathed 100% O2 at 2 ATA for up to 19 hours (Hendricks PL, Hall DA, Hunter WL, Jr., Haley PJ. Extension of pulmonary O2 tolerance in man at 2 ATA by intermittent O2 exposure. J Appl Physiol. 1977;42(4):593-9). Use of 5-minute air breaks after every 20 minutes of 100% O2 delayed the onset of a measurable reduction in vital capacity (-5%) from 6 hours (without air breaks) to 17 hours. We are not aware of any specific studies that look at the influence of air breaks on CNS O2 toxicity. Such a study would be difficult to perform since O2 toxicity is rare.
Air breaks are prescribed in some standard treatment procedures such as USN Treatment Tables for decompression illness. Routine use of air breaks for other hyperbaric treatment algorithms is at the discretion of the treating physician and is often implemented when treatment pressure exceeds 2 ATA. The time or length of the air break can vary from five (5) to ten (10) minutes (up to 15 minutes for treatment protocols used for decompression illness), typically after 100% O2 breathing periods of 20-30 minutes.
Banham ND. Oxygen toxicity seizures: 20 years' experience from a single hyperbaric unit. Diving Hyperb Med. 2011;41(4):202-10
Hadanny, A., Meir, O., Bechor, Y., Fishlev, G., Bergan, J., Efrati, Shai. (2016). The safety of hyperbaric oxygen treatment - retrospective analysis in 2,334 patients. Undersea and Hyperbaric Medicine, 43(2): 113-122
Hampson N, Atik D. Central nervous system oxygen toxicity during routine hyperbaric oxygen therapy. Undersea Hyperb Med. 2003;30(2):147-53
Heyboer M, 3rd, Jennings S, Grant WD, Ojevwe C, Byrne J, Wojcik SM. Seizure incidence by treatment pressure in patients undergoing hyperbaric oxygen therapy. Undersea Hyperb Med. 2014;41(5):379-85
DISCLAIMER
Neither the Undersea and Hyperbaric Medical Society (UHMS) staff nor its members are able to provide medical diagnosis or recommend equipment over the internet. If you have medical concerns about hyperbaric medicine you need to be evaluated by a doctor licensed to practice medicine in your locale, which can provide you professional recommendations for hyperbaric medicine based upon your condition. The responsibility of approving the use of equipment resides with the physician and safety director of the facility. Information provided on this forum is for general educational purposes only. It is not intended to replace the advice of your own health care practitioner and you should not rely upon it as though it were specific medical advice given to you personally.
What is appropriate for treating patient after seizure in chamber? Should every patient who has had seizure be treated with valium? Is it needed if they are alert/talking after treatments and vitals/glucose is normal?
Our patient was a 91 yr old male being treated for osteoradionecrosis. He had a seizure we believe from possible O2 toxicity. He was being treated at 2.5 ATA for 90 min with one 10 minute air break and pressurization rate of 2psi. Seizure happened minutes after his 10 minute air break. Patient did well with air break (given with mask and air tank gauge showed good respiratory effort).
His seizure lasted for ~30 seconds. He never lost consciousness and was alert and talking during decompression and after removal from chamber. He is not diabetic but did check vitals and glucose post tx and all was normal. Patient also had normal vitals, including normal temp prior to tx.
Our NP examined patient pre and post tx. Patient was outpatient so he went home after tx. We do have standing order that we can give 5mg valium for seizures however NP and myself didn’t think it was indicated.
We would like our policy for possible O2 toxicity to be appropriate so your recommendations would be greatly appreciated. What is appropriate for treating patient after seizure in chamber? Should every patient who has had seizure be treated with valium? Is it needed if they are alert/talking after treatments and vitals/glucose is normal?
The responses to the question varied and therefore rather than consolidating them, we are listing them in order of response. Editor
- I have a number of comments. Can you describe this seizure? Was this a focal seizure without LOC? I have never seen that during HBO2, but I guess it can happen. The only ones I have seen were grand mal. This dose of HBO2 seems a little high for this indication. Many years ago we went to 2.0 x 90 minutes (at pressure time) for almost all of wound care and radiation injury and still get good clinical outcomes. Neal authored a letter to the editor in UHM that was convincing that seizures due to HBO2 do not occur at 2.0. Next, HBO2 may have unmasked an occult seizure disorder. I have seen this several times, in which a patient has underlying brain pathology, including occult seizures (“black out spells” the patient later recalled), so this patient needs to be evaluated for this. That evaluation typically includes neurology consult with provocative EEG, exam and MRI. Regarding Valium….If you want seizure prophylaxis for 30 minutes use Valium. If you want it for 2 hours use Ativan. But before using prophylaxis, it would be prudent to work up the patient first. I leave the dosing of HBO2 up to that department, but to my knowledge there is no convincing information about 2.5 ATA being superior to 2.0 ATA. LW
- Dr. LW "said it all" including questioning the type of seizure, obtaining a neurology consultation, treating at 2 ATA pressures, deferring retreatments until cleared by neurology consultant and use of Ativan rather than Valium. MS
- This is a more complicated question than it appears at first glance. First, I agree that the incidence of oxygen toxic seizures during routine hyperbaric treatment performed at a maximum pressure of 2.0 ATA is vanishingly rare. There may have been a couple in the history of the world. This compares to approximately 3-4 in 10,000 routine treatments performed at 2.36 ATA (Welslau 1998, Pflaki 2000, Hampson 2003).
However, the data are not from a population of nonagenarians. I'm not sure if we know whether the extreme elderly are more (or less) susceptible to CNS oxygen toxicity. For that matter, I don't think that we know the response rate to HBO2 with regard to angiogenesis in irradiated tissue in patients of this age.
Secondly, to my knowledge, no hard data have ever been published either in human or animal models demonstrating that benzodiazepines are effective in either preventing or aborting oxygen toxic seizures. When administered prophylactically, it may be a self-fulfilling prophecy because oxygen toxic seizures are so rare, including among patients who have had one previously. The same goes when administering the drugs to abort an oxygen toxic seizure because the seizure will stop whether you administer drugs or not.
Finally, most oxygen toxic seizures are tonic-clonic, but at least one focal seizure has been reported. The article is attached. NH - A few points:
(1). Characterization of the seizure is important. If it was a focal seizure at onset, or as evidenced by Todd’s paralysis afterward, then the patient probably has underlying pathology. Seizures due to O2 exposure alone are generalized at onset, not focal.
(2). In our facility we observe O2 seizures even at 2 ATA, although uncommonly. Around 50% of these are due to concomitant hypoglycemia.
(3). Re-institution of O2 after recovery from the seizure rarely causes a recurrent seizure. Nevertheless, many practitioners administer some sort of anticonvulsant, usually a benzodiazepine. When a seizure occurs in a multiplace facility, the optics of restarting the O2 may appear uncaring to other patients. Thus, locking the patient out of the chamber after the seizure has stopped is a common practice, which also allows for closer assessment and appropriate referral. RM - I agree the story is suspicious of something more than a hyperoxic seizure and needs investigation if it was anything but a generalized seizure.
I was interested to hear the other responses and have a couple of comments:- We also see very occasional seizures but these are (for the last 10 years or so) never associated with hypoglycaemia. That problem seems to have been eliminated with the introduction of an active sugar management program with the diabetic patients.
- We treat as a routine at 2.4 ATA in the multiplace, but after the elimination of a rebreathing phenomenon many years ago, we have come down to a low rate of seizures that we have accepted (right or wrong!). It is about 1:8.000 compressions. I noted Lin's post about treating routinely at 2.0 ATA - we have considered the same but rejected it to date based on the fear we cannot be sure about treatment efficacy given the lower inspired oxygen likely in a multiplace compared to the oxygen-filled monoplace at 2.0 ATA. Perhaps this is illogical and I would welcome more from Lin about how that decision was made.
- I am very interested to hear that many would prescribe benzodiazepines for someone who has suffered a hyperoxic seizure. This is not our practice and has not been a problem to date - touch wood. In our counselling, we are very keen to distance these seizures from any notion of epilepsy and this includes the benefit of benzos or other anticonvulsants.
- Agree with Richard that it is not a good look to try and put the patient back in the same run. In general, the average hyperbaric patient who suffers a hyperoxic siezure takes some time to recover - rather longer than the classic teaching which is presumably based more on fit young male divers in the Navy than octogenerians with multiple pathologies.... MB
- We also see very occasional seizures but these are (for the last 10 years or so) never associated with hypoglycaemia. That problem seems to have been eliminated with the introduction of an active sugar management program with the diabetic patients.
Do you have any information regarding HBOT and concurrent use of chemotheapeutic agents 1) ixabepilone and 2) faslodex?
None of the drugs have a published experience discoverable on a pub med search.
Based on mechanisms of action I doubt any of the drugs wiuld have their toxicities enhanced by HBO2. However, as you know, the decision to treat a patient with HBO2 who is receiving these drugs is the managing physicians decision and our input is meant only to provide guidance based on the information that is discoverable.
Please see the attachment.
Do you have any safety information or contraindications regarding chemo agent Ibrance and concurrent HBOT?
Posted: 12/7/2020
Q:
Do you have any safety information or contraindications regarding chemo agent Ibrance and concurrent HBOT?
A:
Ibrance is a chemotherapeutic drug in the class of drugs called kinase inhibitors. It works to block one or more enzymes that encourage cellular division in the cancer cells. It is used along with an estrogen blocker (typically an aromatase inhibitor) for the treatment of breast cancer.
As for most of the chemotherapeutic drugs there is no published experience of this drug along with HBO2.
Below, I have copied warnings from the manufacturer in regard to a toxicity of the drug that may react unfavorably with HBO2.
Lung problems (pneumonitis). IBRANCE may cause severe inflammation of the lungs during treatment that can lead to death. Tell your doctor right away if you have any new or worsening symptoms, including:
- chest pain
- cough with or without mucus
- trouble breathing or shortness of breath
Your doctor may interrupt or stop treatment with IBRANCE completely if your symptoms are severe.
Since the drug is known to causse pulmonary toxicities in some patients, I recommend that if the patient receives HBO2, on a daily basis they are questioned as to their pulmonary status. I would also recommend that the patient have auscultation of their lungs before and after each treatment.
I do not believe that there is an absolute contraindication to concurrent treatment.
As always the decision to treat is the purview of the treating physician. Our recommendations are given based on the guidance available and we can assume no responsibility for treatinhg an individual patient in whom we do not have the entire history and whom we have not examined.
John J. Feldmeier, D.O.
Question answered by Dr. John Feldmeier, DO
None of the drugs have a published experience discoverable on a pub med search.
Based on mechanisms of action I doubt any of the drugs would have their toxicities enhanced by HBO2. However, as you know, the decision to treat a patient with HBO2 who is receiving these drugs is the managing physicians decision and our input is meant only to provide guidance based on the information that is discoverable
Response to potential Interaction of HBO and the following chemotherapeutic agents:
1.Faslodex (Fulvestrant): This drug is indicated for ER receptor positive breast cancer most often in combination with other agents. It downregulates the expression of the ER receptor and in doing so interferes with tumor growth stimulated by the ER receptor.
It is given as an IM injection monthly.
Its toxicities include asthenia, mild nausea and vomiting, hot flashes, headaches, injection site reactions back pain and arthralgias and a flu like syndrome.
No published experience with its combination with HBO2, but mechanism of action does not appear to be dependent on O2 presence and I doubt any negative interaction of HBO2 with this drug.
- 2. Ixempra (Ixabepilone): This drug is a cell cycle specific agent active during the M-phase of cell division. It inhibits the dynamics of microtubules. It is given IV. Its toxicities include myelosuppression,skin rash, hypotension, flushing, fatigue and asthenia, nausea and vomiting and diarrhea, myalgias, arthralgias and other musculoskeletal pain.
Its mechanism of interaction does not appear to be oxygen dependent. No published experience of interaction with HBO2 was found on literature search.
I doubt that there would be any negative interactions with this drug.
- 3. Ibrance (Palbociclib): This drug is a kinase inhibitor. It interfers with enzymes that promote the activity of certain proteins especially by blocking phosphorylation.
I will append an information sheet on the drug.
No published experience is discoverable with a literature search. Its mode of action does not appea to depend on O2 availabiliity.
I doubt there would be enhanced toxicity with HBO2.
John Feldmeier
Palbociclib
From Wikipedia, the free encyclopedia
(Redirected from Ibrance)
Jump to: navigation, search
|
Palbociclib |
|
|
Clinical data |
|
|
Ibrance |
|
|
· EU EMA: by Palbociclib |
|
|
Legal status |
|
|
· US: ℞-only |
|
|
Identifiers |
|
|
· 6-Acetyl-8-cyclopentyl-5-methyl-2-{[5-(1-piperazinyl)-2-pyridinyl]amino}pyrido[2,3-d]pyrimidin-7(8H)-one |
|
|
Synonyms |
PD-0332991 |
|
PubChem CID |
· 5330286 |
|
· 4487437 |
|
|
· D10372 Y |
|
|
· CHEBI:85993 Y |
|
|
Chemical and physical data |
|
|
C24H29N7O2 |
|
|
447.533 g/mol |
|
|
3D model (Jmol) |
|
|
· O=C2N(c1nc(ncc1/C(=C2/C(=O)C)C)Nc3ncc(cc3)N4CCNCC4)C5CCCC5 |
|
|
· InChI=1S/C24H29N7O2/c1-15-19-14-27-24(28-20-8-7-18(13-26-20)30-11-9-25-10-12-30)29-22(19)31(17-5-3-4-6-17)23(33)21(15)16(2)32/h7-8,13-14,17,25H,3-6,9-12H2,1-2H3,(H,26,27,28,29) · Key:AHJRHEGDXFFMBM-UHFFFAOYSA-N |
|
Palbociclib (codenamed PD-0332991, trade name Ibrance) is a drug for the treatment of ER-positive and HER2-negative breast cancer developed by Pfizer. It is a selective inhibitor of the cyclin-dependent kinases CDK4 and CDK6.[1][2]
Contents
[hide]
Mechanism of action[edit]
Further information: CDK inhibitor
It is a selective inhibitor of the cyclin-dependent kinases CDK4 and CDK6.[1][2]
Approvals and indications[edit]
ER+ breast cancer[edit]
The drug was reviewed and approved under the Food and Drug Administration’s (FDA) accelerated Priority Review and Breakthrough Therapy designation programs on February 3, 2015 as a treatment (in combination with letrozole) for patients with estrogen receptor positive advanced breast cancer.[3] This was an accelerated approval.[4]
In March 2017, the FDA granted regular approval to palbociclib for HER2 negative breast cancer, alongsite an aromatase inhibitor. [5]
A phase 3 trial, PALOMA-2, was fully enrolled by February 2015 and reported positive results in April 2016.[6] The results of PALOMA-2 trial (published November 2016) showed significantly longer progression-free survival in patients on palbociclib in combination with letrozole, compared to patients on letrozole and placebo. Progression-free survival was assessed by radiologically confirmed disease progression by RECIST criteria or death during the study. At the time of publication, there was insufficient data on overall survival, and a final analysis is planned after a total of 390 deaths occur per protocol and in agreement with regulatory agencies. Of note, it was noted that the addition of palbociclib caused higher rates of myelotoxic events in the study.[7]
The drug was approved for use in the European Union in November 2016 as a treatment for hormone receptor (HR) positive, human epidermal growth factor receptor 2 (HER2) negative locally advanced or metastatic breast cancer either in combination with an aromatase inhibitor or, for women who have received prior endocrine therapy, in combination with fulvestrant. In pre- or perimenopausal women, a luteinizing hormone releasing hormone agonist should also be given.[8]
Clinical trials[edit]
HR+ breast cancer[edit]
The PALOMA-3 trial announced in April 2015 that the addition of palbociclib was superior to fulvestrant alone for progression-free survival.[9]
In the phase 2 PALOMA-1 trial reported at the April 2014 annual meeting of the American Association for Cancer Research, the addition of palbociclib to letrozole was shown to significantly slow the progression of advanced cancer (median progression-free survival increased from 10.2 months to 20.2 months), but was not shown to have a statistically significant effect on increasing patients' overall survival times.[10][11][12]
Pricing[edit]
Ibrance "can be ordered through select" specialty pharmacies and "sells for $9,850 for 30 days or $118,200 for a year's supply before discounts."[13] According to a statement by the New York–based Pfizer the price "is not the cost that most patients or payors pay" since most prescriptions are dispensed through health plans, which negotiate discounts for medicines or get government-mandated price concessions.[13] In the United States specialty pharmacies fill prescriptions for drugs that are usually high cost.[14][15]
References[edit]
- ^ Jump up to: a b Finn, RS; Dering, J; Conklin, D; Kalous, O; Cohen, DJ; Desai, AJ; Ginther, C; Atefi, M; et al. (2009). "PD 0332991, a selective cyclin D kinase 4/6 inhibitor, preferentially inhibits proliferation of luminal estrogen receptor-positive human breast cancer cell lines in vitro". Breast cancer research : BCR. 11 (5): R77. PMC2790859 . PMID 19874578. doi:10.1186/bcr2419.
- ^ Jump up to: a b Rocca A, Farolfi A, Bravaccini S, Schirone A, Amadori D (2014). "Palbociclib (PD 0332991): targeting the cell cycle machinery in breast cancer". Expert Opin Pharmacother. 15 (3): 407–20. PMID24369047. doi:10.1517/14656566.2014.870555.
- Jump up ^ "FDA Approves Palbociclib for Metastatic Breast Cancer". OncLive. 3 Feb 2015.
- Jump up ^ "Pfizer Receives U.S. FDA Accelerated Approval of IBRANCE (palbociclib)". Pfizer. 3 Feb 2015.
- Jump up ^ cite web | url=https://www.fda.gov/Drugs/InformationOnDrugs/ApprovedDrugs/ucm549978.htm
- Jump up ^ Late-stage study of expanded use of Pfizer's Ibrance successful; global regulatory applications to follow. April 2016
- Jump up ^ Finn; et al. (November 17, 2016). "Palbociclib and Letrozole in Advanced Breast Cancer". NEJM. pp. 1925–1936. doi:10.1056/NEJMoa1607303.CS1 maint: Explicit use of et al. (link)
- Jump up ^ Ibrance (palbociclib) European public assessment report
- Jump up ^ "Pfizer Announces PALOMA-3 Trial For IBRANCE (Palbociclib) Stopped Early Due To Efficacy Seen In Patients With HR+, HER2- Metastatic Breast Cancer Whose Disease Has Progressed Following Endocrine Therapy". April 15, 2015.
- Jump up ^ Breast Cancer Drug Shows ‘Groundbreaking’ Results By ANDREW POLLACK, APRIL 6, 2014
- Jump up ^ Beasley, Deena (6 April 2014). "Pfizer drug doubles time to breast cancer tumor growth in trial". Yahoo! News. Reuters. Retrieved 7 April 2014.
- Jump up ^ Palbociclib Shows Promising Results in Patients With Hormone Receptor-positive Metastatic Breast Cancer, AACR in the News, April 6, 2014
- ^ Jump up to: a b "Pfizer breast cancer drug gets early FDA approval". Daily Mail. London. Associated Press. 3 February 2015. Retrieved 2 November 2015.
- Jump up ^ Herper, Matthew (19 February 2010), "The World's Most Expensive Drugs", Forbes, retrieved 25 June 2015
- Jump up ^ Thomas, Kate; Pollack, Andrew (15 July 2015). "Specialty Pharmacies Proliferate, Along With Questions". Sinking Spring, Pa.: New York Times. Retrieved 5 October 2015.
|
[hide] |
|||||||
|
CI monoclonal antibodies ("-mab") |
|
||||||
|
Tyrosine-kinase inhibitors ("-nib") |
|
||||||
|
Other |
|
||||||
<img src="//en.wikipedia.org/wiki/Special:CentralAutoLogin/start?type=1x1" alt="" title="" width="1" height="1" style="border: none; position: absolute;" />
Retrieved from "https://en.wikipedia.org/w/index.php?title=Palbociclib&oldid=789468781"
Can you clarify? For dx of DFU 3 or higher, one of the qualifiers for HBO is that patient failed 30 days of wound care. If the patient''s wound was only a DFU 2 during those 30 days, does that count or does the wound need to be a DFU 3 during those 30 days?
CMS clearly states must be Wagner Grade III or higher. See links below for the NCD and also for the UHMS CPG for Diabetic Foot Ulcer.
- National Coverage Determination (NCD) for Hyperbaric Oxygen Therapy (20.29)
- A clinical practice guideline for the use of hyperbaric oxygen therapy in the treatment of diabetic foot ulcersin the treatment of diabetic foot ulcers
UHM 2015, Vol. 42, No. 3
CPG Authors: Enoch T. Huang, Jaleh Mansouri, M. Hassan Murad, Warren S. Joseph, Michael B. Strauss, William Tettelbach, Eugene R. Worth
UHMS CPG Oversight Committee: Enoch T. Huang, John Feldmeier, Ken LeDez, Phi-Nga Jeannie Le, Jaleh Mansouri, Richard Moon, M. Hassan Murad
CORRESPONDING AUTHOR: Dr. Enoch T. Huang – enoch.huang@mac.com
The question concerns a 49-year-old otherwise healthy woman who presented in 2017 with complaints of progressive noise magnification and severe headaches.
There are several anecdotal reports of HBO2 for brain necrosis. In some radiosurgery series, the incidence of brain necrosis is as high as 25%.As with all CNS injuries early intervention is likely to have a higher rate of success. Determinants of outcome obviously include neurologic symptom response, but some series report decreases in steroid requirements and improvement on brain imaging mostly MRI. In my reading of the literature Avastin does not give consistent response.
I would recommend at least 40 treatments at 2.4 ATA. Many patients appear to require a good number of treatments for sustainable response, perhaps well over 60.To my knowledge no one has reported a higher likelihood of seizures during HBO with this group. If seizure activity is part of the picture adequate coverage with anti-convulsants is obviously needed.
See the below abstract and some pdf of slides from one of my presentations.
John Feldmeier
- Hyperbaric oxygen treatment for post-radiation central nervous system injury: a retrospective case series.
Undersea Hyperb Med. 2014 Mar-Apr;41(2):87-96.
Valadão J, Pearl J, Verma S, Helms A, Whelan H. -
CNS-Brain Necrosis
John Feldmeier, DO
61 year old patient with bilateral optic neuropathy secondary to radiation. Has recently been started on prednisone 80mg daily, vitamin E 1000U daily, and pentoxifylline 400mg TID by neuro-ophthalmology. I know the steroids can increase oxygen toxicity, but that the Vitamin E also decreases this risk. Not sure if they offset each other. No seizure history, no pulmonary history, no history of tobacco use. Plan would be 90 minutes at 2.0 ATA with one 5 minute air break? Should number of air breaks be
Other history: Previously healthy male diagnosed with grade 4 glioblastoma 10/2017 s/p resection and chemoradiation (completed 1/2018). Loss of visual acuity bilaterally x 4 weeks, with nearly complete loss of vision on the right. MRI consistent with radiation optic neuropathy. Patient hoping to preserve what vision he has left. Understands data is limited. Also noteworthy, patient has a known atrial septum defect with bidirectional shunting.
A: Treatment for this disorder is recommended. I am always in favor of 2.4 ATA for treatment of radiation injuries especially of the CNS. Many if not most of these patients are on steroids. In the fairly large series from Laurie Gesell while at U of Cincinnati, these folks were not prone to O2 related seizure though certainly this can happen. The known septal defect is not an issue because we are not talking about an air dive. Treatment with Vitamin E might offer some slight protection. If I were to treat this patient, I would treat 3 30 min periods with 5 minute airbreaks at 2.4 ATA and only depart from this if there was a seizure. Informed consent of course is important. This profile chosen because of the severity of the condition and the track record in treating radiation injuries at 2.4 ATA-also the animal study by Marx et al. The profile you suggest is certainly safe but may not be as effective.
John Feldmeier, DO
Anybody have any experience treating pneumocephaly (complication of epidural injection) with HBOT?
Unless there is a clinical problem besides the presence of air (while will resolve on its own), I see no reason to treat. If there is a desire to accelerate resolution, 100% O2 administration at 1 ATA will do that.
Is there any salutary effects for the use of HBO in aggressive glioblastoma ?
As yet, there are no approved or reimbursed indications for HBO2 and the treatment of GBM or the complications of its treatment except for the treatment of radiation necrosis. Please see the attached. It comes from a draft of the about to be published update of the Indications BOOK (HBO2 Committee Report). As such it is unpublished data,.and as such its reproduction is prohibited.
John Feldmeier
Has there been any research to see if there are contraindications to a female patient being dove to 2.4 ATA with a Mirena IUD in place? Will the change in ATA cause an increase or decrease in hormone delivery? (Currently 20mg/24 hrs over 5 years) and 2nd, will the change in ATA increase the risk that the IUD will migrate to perferate the uterus?
Date Posted: 3/11/2020
MEDFAQ Question: Has there been any research to see if there are contraindications to a female patient being dove to 2.4 ATA with a Mirena IUD in place? Will the change in ATA cause an increase or decrease in hormone delivery? (Currently 20mg/24 hrs over 5 years) and 2nd, will the change in ATA increase the risk that the IUD will migrate to perferate the uterus?
Thank you for your question. The UHMS HBO2 safety committee can provide information to assist you in answering your question, but the ultimate responsibility for these types of questions rests with the medical director and safety director of your facility.
Generally speaking, intrauterine devices are an effective and popular form of birth control. Based upon the frequency of their use, hyperbaric professionals should be prepared to field questions related to the safety of these devices within the unique environment of the hyperbaric chamber.
For the sake of clarity, there are two types of IUDs:
Non-hormonal IUD: These devices are made of copper and may last up to twelve years.
Hormonal IUD: These devices are designed to release small amounts of hormone (typically levonorgestrel) locally into the uterus. Levonorgestrel causes thickening of the cervical mucus and thins the lining of uterus.
In particular, the Mirena IUD is a hormonal IUD that is made of soft, flexible plastic and does not appear to contain gas spaces that could be affected by changes in atmospheric pressure. As such, the rate of hormone release would theoretically remain unchanged. Furthermore, increased atmospheric pressure at standard hyperbaric oxygen therapy pressures between 2.0 and 3.0 ATA is not expected to increase the risk of uterine wall perforation. Unfortunately, there are no confirmed studies, reports or testing of this product by the manufacturer under hyperbaric conditions that would validate these suppositions.
The UHMS Hyperbaric Oxygen Safety Committee therefore suggests that a risk assessment be conducted by the Safety Director and Medical Director of the Hyperbaric Facility for your particular patient. There are several related references that may assist you in completing the risk assessment and determining the proper course of action. Of note, the Divers Alert Network has responded to several inquiries related to these devices from a commercial or scuba diving perspective. Their position pertaining to intrauterine devices and diving is that an increase in absolute barometric pressure should have no mechanical effect on the IUD, and there is probably no reason to suspect their hormonal bioavailability or metabolism should be affected. The proportion of female divers diving with a IUD should be no different than that of general population, and DAN has never been made aware of any issues with IUD devices, medicated or not.
Related Articles:
http://www.alertdiver.com/womens_health_and_diving
https://www.diversalertnetwork.org/medical/articles/DAN_Explores_Fitness_and_Diving_Issues_for_Women
http://midlandsdivingchamber.co.uk/index.php?id=advice&page=6&cat=10&sub_cat=11
Respectfully,
The UHMS Safety Committee
DISCLAIMER
Neither the Undersea and Hyperbaric Medical Society (UHMS) staff nor its members are able to provide medical diagnosis or recommend equipment over the internet. If you have medical concerns about hyperbaric medicine you need to be evaluated by a doctor licensed to practice medicine in your locale, which can provide you professional recommendations for hyperbaric medicine based upon your condition. The responsibility of approving the use of equipment resides with the physician and safety director of the facility. Information provided on this forum is for general educational purposes only. It is not intended to replace the advice of your own health care practitioner and you should not rely upon it as though it were specific medical advice given to you personally.
HBOT for COVID Cytokine storm 1 )It is reported patients suffering from COVID-19 have elevated levels of many cytokines (IL-1,2,4,7,10,12,13,17, GCSF, TNF, others). Could HBOT not down regulate this response to mitigate the resultant ARDS? If so, should HBOT be implemented in patients not yet intubated but at risk, and how do we identify? Or should it be used for those with ARDS on vent support, and when to initiate, early or late? 2) Aside from the cytokine storm question, what of the role of HBOT in
Posted 4/3/2010
Q: HBOT for COVID Cytokine storm
1 )It is reported patients suffering from COVID-19 have elevated levels of many cytokines (IL-1,2,4,7,10,12,13,17, GCSF, TNF, others). Could HBOT not down regulate this response to mitigate the resultant ARDS?
If so, should HBOT be implemented in patients not yet intubated but at risk, and how do we identify?
Or should it be used for those with ARDS on vent support, and when to initiate, early or late?
2) Aside from the cytokine storm question, what of the role of HBOT in the supportive role of mitigating hypoxic end organ injury?
A:
The UHMS website has an extensive section addressing the issue of HBO2 for COVID-19. The portion of this posting that deals with the rationale for treatment including mechanisms extensively deals with the questions asked above. We do indeed believe that HBO2 can have a favorable impact on the cytokine storm and especially through its anti-inflammatory effects reduce the exaggerated immune response that is at the heart of damage caused by the infection. Please refer to this posting.
HBOT for COVID Cytokine storm: Is there any reasonably valuable anecdotal evidence of HBOT benefit for COVID-19 or Sars-1?
Posted 4/3/2020
Q:
HBOT for COVID Cytokine storm: Is there any reasonably valuable anecdotal evidence of HBOT benefit for COVID-19 or Sars-1?
A:
The UHMS website has an extensive section addressing the issue of HBO2 for COVID-19. The portion of this posting that deals with the rationale for treatment including mechanisms extensively deals with the questions asked above. We do indeed believe that HBO2 can have a favorable impact on the cytokine storm and especially through its anti-inflammatory effects reduce the exaggerated immune response that is at the heart of damage caused by the infection. Please refer to this posting.
What are the current guidlines for a non insulin dependent patient in a monoplace chamber?
Posted: 4/22/2020
We do not have guidelines for the management of diabetics in the chamber however there are a number of resources available to you, including the attached BNA Nursing Guidelines, Best Publishing’s Policy and Procedural Guidelines for Hyperbaric Facilities (2022) published a recommended scale in policy #304 on page 51 and Best Publishing Company’s Hyperbaric Medicine Practice, 4th Edition (2017) on page 126 in the Hyperbaric Nursing chapter and on page 144 in The Use of Drugs Under Pressure chapter, the topic is covered.
I had COVID-19. Will I be able to return to diving?
Posted: 4/23/2020
QUESTION:
I had COVID-19. Will I be able to return to diving?
ANSWER:
At the present time, we simply do not have sufficient data to support or refute the definitive proclamations made by this case series. Any attempt to generalize the effects of COVID-19 based upon a single case series (6-cases) published in the lay-press1,2, should be met with appropriate scrutiny.
Covid-19 symptoms range from mild to severe. Some people have no symptoms at all while others require complicated stays in an intensive care setting and require ventilatory support. The recent report published in the lay-press1,2 has resulted in considerable concern related to the finding of pulmonary inflammation in mild cases of COVID-19. This case series reports findings that may provide some insight into post-infection recovery, with a potential knock-on effect on fitness to dive evaluations, and recommendations related to medical follow up studies, and convalescence period prior to a return to diving. However, we must interpret this small case series (6-cases) with caution, as there is not enough known about the natural history of this disease to confidently extrapolate prognostic guidance from this one report, nor generalize these findings to every case of COVID-19. Likewise, calls for a particular medical examination or screening test(s) following infection to determine fitness to dive, based on this work alone, are currently unsubstantiated and premature.
The list of potential variables related to how this disease manifests, its clinical course, and longterm prognosis is lengthy and may include factors such as underlying medical conditions, age, disease severity, and secondary complications. Case reports suffer from multiple design weaknesses to include a lack of controls and randomization, which makes any conclusions that we may want to generalize to a larger population suspect. While these findings are indeed disquieting, it will take time before the potential impact on individual health, and any lasting effects on lung or heart function, are captured in the peer-reviewed literature.
COVID-19 shares many of the same features as other serious viral pneumonias that require a period of convalesce before returning to full activities – a process that can take weeks or months depending on symptom severity. The long-term effects of COVID-19 on pulmonary function and recovery time will vary, and there is insufficient experience and sound clinical research to make accurate prognostic determinations.
As the diving medical community gains more experience, and has the opportunity to study this illness and follow patients through their recovery, we will develop a thoughtful approach to making fitness to dive determinations. A single small case series is insufficiently powered to support definitive statements related to permanent lung function changes or air trapping risk – but these are unquestionably areas of keen interest within the diving medical community and will be closely monitored.
Over the next several months, the global medical community will gain a better understanding of the natural history of this disease. In addition, multiple studies are underway looking at treatment modalities and how we may reduce morbidity and mortality. COVID-19 has gripped the world and there is no other time in our history where we have as many people searching for answers about a single disease. We will continue to track research on this topic and update this position as new information becomes available.
_________________________________
- Hartig, Frank. Tauchen nach Covid-19-Erkrankung? Wetnotes. April 15, 2020. https://www.wetnotes.eu/tauchen-nach-covid-19-erkrankung/
- (Translation of reference 1). Bandera County Courier. Medic sees evidence of serious long-term lung damage. April 18, 2020. https://www.bccourier.com/medic-sees-evidence-of-serious-long-term-lung-damage/
- Hughes, Russel. COVID-19 potential impact on divers. Advanced Diving NZ. April 21, 2020. https://www.advanceddivingnz.com/advanced-diving-blog/2020/4/21/covid-19-potential-impact-on-divers?fbclid=IwAR2bhP-kXvUYCKNQu8a-tpzlMQf6YKX2m1AlPlYYZadEYrWGZKu0sroTCEk.
A recent article, “Tauchen nach Covid-19-Erkrankung?” concludes that divers who have had COVID-19 will be permanently unfit to dive. Is this opinion shared by diving medical professionals? What is the evidence?
Posted: 4/24/2020
QUESTION:
A recent article, “Tauchen nach Covid-19-Erkrankung?” concludes that divers who have had COVID-19 will be permanently unfit to dive. Is this opinion shared by diving medical professionals? What is the evidence?
ANSWER:
At the present time, we simply do not have sufficient data to support or refute the definitive proclamations made by this case series. Any attempt to generalize the effects of COVID-19 based upon a single case series (6-cases) published in the lay-press1,2, should be met with appropriate scrutiny.
Covid-19 symptoms range from mild to severe. Some people have no symptoms at all while others require complicated stays in an intensive care setting and require ventilatory support. The recent report published in the lay-press1,2 has resulted in considerable concern related to the finding of pulmonary inflammation in mild cases of COVID-19. This case series reports findings that may provide some insight into post-infection recovery, with a potential knock-on effect on fitness to dive evaluations, and recommendations related to medical follow up studies, and convalescence period prior to a return to diving. However, we must interpret this small case series (6-cases) with caution, as there is not enough known about the natural history of this disease to confidently extrapolate prognostic guidance from this one report, nor generalize these findings to every case of COVID-19. Likewise, calls for a particular medical examination or screening test(s) following infection to determine fitness to dive, based on this work alone, are currently unsubstantiated and premature.
The list of potential variables related to how this disease manifests, its clinical course, and longterm prognosis is lengthy and may include factors such as underlying medical conditions, age, disease severity, and secondary complications. Case reports suffer from multiple design weaknesses to include a lack of controls and randomization, which makes any conclusions that we may want to generalize to a larger population suspect. While these findings are indeed disquieting, it will take time before the potential impact on individual health, and any lasting effects on lung or heart function, are captured in the peer-reviewed literature.
COVID-19 shares many of the same features as other serious viral pneumonias that require a period of convalesce before returning to full activities – a process that can take weeks or months depending on symptom severity. The long-term effects of COVID-19 on pulmonary function and recovery time will vary, and there is insufficient experience and sound clinical research to make accurate prognostic determinations.
As the diving medical community gains more experience, and has the opportunity to study this illness and follow patients through their recovery, we will develop a thoughtful approach to making fitness to dive determinations. A single small case series is insufficiently powered to support definitive statements related to permanent lung function changes or air trapping risk – but these are unquestionably areas of keen interest within the diving medical community and will be closely monitored.
Over the next several months, the global medical community will gain a better understanding of the natural history of this disease. In addition, multiple studies are underway looking at treatment modalities and how we may reduce morbidity and mortality. COVID-19 has gripped the world and there is no other time in our history where we have as many people searching for answers about a single disease. We will continue to track research on this topic and update this position as new information becomes available.
_________________________________
- Hartig, Frank. Tauchen nach Covid-19-Erkrankung? Wetnotes. April 15, 2020. https://www.wetnotes.eu/tauchen-nach-covid-19-erkrankung/
- (Translation of reference 1). Bandera County Courier. Medic sees evidence of serious long-term lung damage. April 18, 2020. https://www.bccourier.com/medic-sees-evidence-of-serious-long-term-lung-damage/
- Hughes, Russel. COVID-19 potential impact on divers. Advanced Diving NZ. April 21, 2020.https://www.advanceddivingnz.com/advanced-diving-blog/2020/4/21/covid-19-potential-impact-on-divers?fbclid=IwAR2bhP-kXvUYCKNQu8a-tpzlMQf6YKX2m1AlPlYYZadEYrWGZKu0sroTCEk.
I have a patient that I am trying to get approved for HBO. His radiation dose was 5040 over 28 treatments to his pelvis for colorectal CA. Is he a good candidate based on his dose? It seems that it may be a bit low (thinking 6000 cut off).
Posted: 6/24/2020
Q: I have a patient that I am trying to get approved for HBO2. His radiation dose was 5040 over 28 treatments to his pelvis for colorectal CA and is having continuous perianal skin breakdown for one year. Is he a good candidate based on his dose? It seems that it may be a bit low (thinking 6000 cut off).
A: The perineal area when included in the treatment volume is a tough area to heal. I think the dose is adequate to cause these problems and the material fact is that there are non-healing tissues and that they are persistent at a year.
A patient that is likely going to start HBO2 soon, presented a model number of his intraocular lens implant (MI60L). While I think this is okay, I would like to check since he has the model number from Bausch & Lomb. How can I determine if this posterior chamber implant is compatible with HBO2 Therapy?
Posted: 7/1/2020
Q:
A patient that is likely going to start HBO2 soon, presented a model number of his intraocular lens implant (MI60L). While I think this is okay, I would like to check since he has the model number from Bausch & Lomb. How can I determine if this posterior chamber implant is compatible with HBO2 Therapy?
A:
Most of the issues of eye surgery and immersed diving are largely irrelevant in the dry hyperbaric environment unless there are intraocular gas bubbles as mentioned below.
Air bubbles are sometimes present in the eye for a few days after cataract surgery and their absence should be specifically documented by the ophthalmologist prior to HBO2 if the HBO2 takes place shortly after cataract surgery.
There is no physiological reason that I am aware of that would mandate a waiting period for an HBO2 treatment after cataract surgery in the absence of an intraocular gas bubble.
I am unaware of any reports of negative effects of HBO2 on intraocular lens implants. I have also never heard of patients who have intraocular lens implants experiencing a myopic shift as a result of HBO2 treatments, as many patients with their natural lens still in place do.
As always, I would suggest that the patient discuss this information with the ophthalmologist responsible for their care.
I would like to start my 57-year-old patient on HBO therapy for soft tissue radiation injury. He completed chemotherapy and radiation for treatment of rectal cancer about 21 months ago. Since that time, he struggled with perianal cutaneous ulcers. I think HBO will help. I want to make sure the FOLFOX and 5-FU chemotherapy he completed 21 months ago does not complicate his case. I do not think they do, I am sure they have cleared his system.
Posted: 7/6/2020
Q:
I would like to start my 57-year-old patient on HBO therapy for soft tissue radiation injury. He completed chemotherapy and radiation for treatment of rectal cancer about 21 months ago. Since that time, he struggled with perianal cutaneous ulcers. I think HBO will help. I want to make sure the FOLFOX and 5-FU chemotherapy he completed 21 months ago does not complicate his case. I do not think they do, I am sure they have cleared his system.
A:
None of the drugs in the FOLFOX multi-drug protocol given nearly 2 years ago should complicate your intent to give HBO2
for perianal ulcers, presumably caused by radiation.
Please, remember that the cancer itself can cause fistulas to the skin of the perineum. Just cautioning that you make sure that he has no active cancer because the cancerous wounds will not heal using HBO2.
I am currently treating a patient with breast cancer for a lower extremity wound due to late effects of radiation. Ibrance has been held due to known effects on wound healing. She has completed #20 HBOT. Wound has shown some improvement, but not yet resolved. Patient's oncologist would like to resume Ibrance. Are there any relative or absolute contraindications to continuing HBOT once Ibrance is resumed?
Posted: 7/14/2020
Q:
I am currently treating a patient with breast cancer for a lower extremity wound due to late effects of radiation. Ibrance has been held due to known effects on wound healing. She has completed #20 HBOT. Wound has shown some improvement, but not yet resolved. Patient's oncologist would like to resume Ibrance. Are there any relative or absolute contraindications to continuing HBOT once Ibrance is resumed?
A:
Please see the following paper: Ibrance (Palbociclib) and Hyperbaric Oxygen
It does look like this drug might interfere with wound healing although probably no more so than many other chem drugs. There is nothing found on a literature search of the two together.
I would predict no enhancement of toxicity with the caution that without any published experience that prediction is no more than an educated guess based on a review of the drug's characteristics. As I always try to do, I also add the caution that the treating physician must take responsibility for any unexpected enhanced toxicities when HBO2 is given to a patient on this drug.
How long do the effects of HBO for osteoradionecrosis last? E.g. a patient was treated for ORN (40 sessions) four years ago, needs repeat oral surgery, would warrant re-treatment with Marx protocol 20+10? What about if it was only 2 years ago?
Posted: 7/31/2020
Q:
Title: How long do the effects of HBO for osteoradionecrosis last? E.g. a patient was treated for ORN (40 sessions) four years ago, needs repeat oral surgery, would warrant re-treatment with Marx protocol 20+10? What about if it was only 2 years ago?
A:
Bob Marx is of the opinion that once a patient completes a full course of HBO2 he or she does not need to repeat again EXCEPT if there is actual radionecrosis. If it is to support a dental extraction or implant, there would be no need for more HBO2. Bob Johnson who has been Bob Marx's collaborator on much of their joint efforts would say that if at the time of the oral surgery the tissues did not appear well-vascularized, it would be appropriate to give 10 post procedure treatments but with out the pre-op sessions. BUT, if there is bony necrosis present a second full 30 and 10 would be the best course.
In a person with heavy alcohol dependence, is there a concern of alcohol withdrawal seizures during HBO therapy for a different condition (i.e. STRN, etc)? If so, has this risk been described or quantified, and would expert consensus recommend using a specific chamber class (multiplace vs monoplace) to treat an approved indication, given this comorbidity? Thank you.
Posted: 8/11/2020
Q:
In a person with heavy alcohol dependence, is there a concern of alcohol withdrawal seizures during HBO therapy for a different condition (i.e. STRN, etc)? If so, has this risk been described or quantified, and would expert consensus recommend using a specific chamber class (multiplace vs monoplace) to treat an approved indication, given this comorbidity?A:
A:
In regard to dealing with alcohol withdrawal and hyperbaric treatment for non-emergent indications, it seems to me that the most prudent course of action is to delay treatment until the patient has gone through the process of withdrawal with all its attendant physiologic and neuropsychiatric problems. I personally would not want to deal with a patient in the chamber in this state. After the process of withdrawal has been completed the patient should be fine for treatment. Just as in other patients, if he or she is agitated or claustrophobic, a benzodiazepine anxiolytic would be in order.
Many alcoholic patients have been treated with HBO2 over the years. Although alcohol abuse may theoretically reduce threshold for seizure activity, it has not been a common problem.
Below is an abstract that suggests based on very limited anecdotal experience that alcohol withdrawal may lower the threshold for O2 induced seizure.
Risk Factors for Oxygen Toxicity Seizures in Hyperbaric Oxygen Therapy: Case Reports From Multiple Institutions
Ruthanna Seidel 1, Christopher Carroll 2, Debra Thompson 2, Rena G Diem 2, Kwabena Yeboah 2, A J Hayes 2, Brett Hall 2, Harry T Whelan 2
Affiliations
· 1University of Arizona College of Medicine, Phoenix, Phoenix, Arizona, USA.
· 2Medical College of Wisconsin, Milwaukee, Wisconsin, USA.
· PMID: 24377194
Abstract
Oxygen toxicity seizures are a rare but recognized complication of hyperbaric oxygen (HBO2) therapy. Many patients undergoing HBO2 therapy have medical conditions or are taking medications that could contribute to seizures. Previous literature has not extensively reported on these factors in patients experiencing oxygen toxicity seizures. We conducted a chart review at several hyperbaric oxygen centers in the Milwaukee, Wisc., area to explore whether the patients who experienced seizures in the hyperbaric chamber had other medical comorbidities or were on medications which lowered their seizure threshold, thereby contributing to oxygen toxicity seizures. There were a total of seven cases of seizures in five patients. Each patient had risk factors for seizures, including hypercapnia secondary to chronic obstructive pulmonary disease, narcotic withdrawal, alcohol dependence, and antidepressant, tramadol or cephalosporin/ceftriaxone use. We hypothesize that patients who experience oxygen toxicity seizures may have other factors which contribute to the development of these seizures.
My partner and I are working on an HBO safety profile for a patient that may benefit from HBO. The patient is currently treated with cabazitaxel. Please see details below and if you have time, please weigh in as to the safety of this chemo and HBO combination.
Posted: 8/27/2020
Q:
My partner and I are working on an HBO safety profile for a patient that may benefit from HBO. The patient is currently treated with cabazitaxel. Please see details below and if you have time, please weigh in as to the safety of this chemo and HBO combination.
He is a 68 year old seeking HBOT for radiation proctitis and radiation cystitis with hematuria in the setting of chronic anticoagulation (Eliquis) for history of PE. Metastatic disease to lymph nodes currently treated with cabazitaxel every three weeks. Has been tolerating this well (has undergone 11 cycles to date) and associates treatment symptoms with Neulasta.
A:
This particular drug was not used commonly in my experience but it may have become more popular since I have retired. On of its indications is for prostate cancer. Prostate cancers do not respond to chemotherapies well in general and this drug is second line even for that tumor. It interferes with the mitosis of cancer cells by interfering with the disassembly of the microtubules which is necessary for the movement of the chromosomes during mitosis to 2 poles to allow for cellular division. My reference textbook says that 80% of the drug has been eliminated from the body within 2 weeks of an IV infusion. Its main side effects are blood count suppression, mausea and vomiting, fatigue, peripheral nerve toxicity, myalgias and arthralgias, cardiac toxicities, hematuria and dysuria. This drug itself can cause hematuria. I am assuming your patient has had radiation? If so the hematuria is complex with the drug, radiation and anti-coagulants all contributing to the hematuria and making it more likely to be refractory to treatment.
See link below for one abstract where Taxol (the original Taxane) was used in a clinical protocol with HBO. It would appear to me that your patient is not receiving concurrent chemotherapy but has had the drug before.
I don't think that there is a high likeihood of worsened side effects with HBO.John Feldmeier, DO
Systemic chemotherapy using paclitaxel and carboplatin plus regional hyperthermia and hyperbaric oxygen treatment for non-small cell lung cancer with multiple pulmonary metastases: preliminary results
Takayuki Ohguri 1, Hajime Imada, Hiroyuki Narisada, Katsuya Yahara, Tomoaki Morioka, Keita Nakano, Yasuhiro Miyaguni, Yukunori Korogi
Is vitamin E is a reasonable approach to preventing oxygen toxicity seizures in a patient on chronic prednisone?
Posted: 9/3/2020
Q:
Is vitamin E is a reasonable approach to preventing oxygen toxicity seizures in a patient on chronic prednisone?
A:
There is no current evidence that Vitamin E is an appropriate prophylactic in mitigating CNS oxygen toxicity during HBO2, and there is also no reported evidence that steroids increase CNS oxygen toxicity risk during HBO2.
We treated a patient recently with hemorrhagic cystitis secondary to BK virus.(40 treatments, 6/11/20-8/11/20) He has a history of CML. In the last 2-3 weeks the patient has had a recurrence of hematuria "dependent on hydration" and the team has reached out to us for more treatments. Do you think more treatments would be efficacious?
Posted: 10/16/2020
Q:
We treated a patient recently with hemorrhagic cystitis secondary to BK virus.(40 treatments, 6/11/20-8/11/20) He has a history of CML. In the last 2-3 weeks the patient has had a recurrence of hematuria "dependent on hydration" and the team has reached out to us for more treatments. Do you think more treatments would be efficacious?
A:
I did a search and have seen Dr. Moon's reply. As he said there may be a role for hyperbaric oxygen in hemorrhagic cystitis in leukemic patients who have stem cell transplants for their leukemia. In my reading up to 50% of such patients sustain cystitis and there appears to be no other effective therapies. The cystitis is viral in etiology (polyoma virus). I attach 3 abstracts of small series of cases treated with HBO2. with a good reported response. I note that they typically report response after about 10 treatments. I did not see that patients have received more than 40 treatments.
- Hemorrhagic cystitis due to polyomavirus abstracts
- Clinical effectiveness of hyperbaric oxygen therapy for BK-virus-associated hemorrhagic cystitis after allogeneic bone marrow transplantation
J Savva-Bordalo1, C Pinho Vaz1, M Sousa1, R Branca1, F Campilho1, R Resende2, I Baldaque3, O Camacho2 and A Campos1
Bone Marrow Transplantation (2012) 47, 1095 -- 1098 & 2012 Macmillan Publishers Limited All rights reserved 0268-3369/12
www.nature.com/bmt
We have been treating a pt. with radiation cystitis and his main symptom is extreme pain with urination and also defecation. We are nearing completion of 40 treatment at 2.4 ata x90 minutes. Like oking at our LCD, it says that treatments must be completed in 4-8 weeks. This patient has had absolutely no changes in symptoms. Has anyone achieved results going beyond 40 treatments? Is it even possible to go beyond 40 and have insurance approve it?
Posted: 12/7/2020
Q:
We have been treating a pt. with radiation cystitis and his main symptom is extreme pain with urination and also defecation. We are nearing completion of 40 treatment at 2.4 ata x90 minutes. Like oking at our LCD, it says that treatments must be completed in 4-8 weeks. This patient has had absolutely no changes in symptoms. Has anyone achieved results going beyond 40 treatments? Is it even possible to go beyond 40 and have insurance approve it?
A:
We had two physician experts comment on your questions, Drs. John Feldmeier and Helen Gelly. Both were kind enough to share their knowledge and experiences that we hope you’ll share with your physician team members. Additionally, Dr. Feldmeier has several questions to help us better understand the clinical situation.
My experience has been that radiation cystitis is often refractory or at least slow to respond to HBO2 treatment and commonly requires more than 40 treatments. I know of several cases treated to 60 plus and even 90 treatments before signs and symptoms resolved. I have also seen several cases where patient have recurred with hematuria in a few months post initial treatment and good initial response. These usually will respond to a second course of HBO2
When you say the patient has not improved, have you been tracking any objective signs? If the patient had had any anemia, is this improving? If the patient had required transfusion previously, has this improved? Has the hematuria improved? Is the patient on anti-coagulants for atrial fibrillation or following deep venous thrombosis or PE? Has the patient had cystoscopy?
I would review the patient's meds and see if any of them tend to cause abnormal bleeding. If they can be decreased in dose or preferably D/Ced, I would do so after the concurrence of the physician who started the meds. I also recommend that the patient have a cystoscopy at this time. You need this to make sure that there is no malignancy causing the bleeding and also if there is one or just a few troublesome sites a local electrocautery or laser photo coagulation might be in order. At any rate having a direct visualization and comparison if cystoscopy was done prior to HBO2 will give valuable information as to whether there has been an improvement. This information may also help in making a case to the insurer for more HBO2 if some improvement is seen.. Again, in my experience, often cystitis requires more than 40 treatments, but if there truly has been no response other causes or complicating factors need to be considered.
The first thing is that I would have the urologist do another cystoscopy. With bladders and bowel you are truly blind as to progress, and unless you are following them closely you can miss a local recurrence or a new primary. Also, from a payment standpoint, if you are going to exceed 60, you better have evidence of improvement, and the only way to do that is to scope them.
I would be concerned that there is not a greater impact at 40.
From a payment perspective, after 60, they need to be prepared to defend any more treatments, and that will require independent evidence.
And I agree that you have to rule other causes of persistent bleeding and pain ( all of John's suggestions are excellent), we had one guy that got better through the week and then would come back worse after the weekend and we finally figured out that he would not hydrate (to decrease urination) and then ride his lawnmower for hours over rough terrain. But that is anecdotal.
For patients with a history of seizure(s), is there literature to define their risk for an O2-induced seizure? Is there any sort of consensus on how to alter a treatment protocol such as increased number of air breaks or treatment depth? Are there thresholds to clear to treat such as length of time to be seizure-free (on or off antiseizure meds)? Or is such a patient at the same risk as any other patient? I realize that each seizure patient may be different (focal vs. generalized and not a question of rem
Posted : 12/7/2020
Q:
For patients with a history of seizure(s), is there literature to define their risk for an O2-induced seizure? Is there any sort of consensus on how to alter a treatment protocol such as increased number of air breaks or treatment depth? Are there thresholds to clear to treat such as length of time to be seizure-free (on or off antiseizure meds)? Or is such a patient at the same risk as any other patient? I realize that each seizure patient may be different (focal vs. generalized and not a question of remote h/o febrile seizure in childhood).
For patients with a history of seizure(s), is there literature to define their risk for an O2-induced seizure?
- Hyperbaric Oxygen Therapy: Side Effects Defined and Quantified; Marvin Heyboer III,* Deepali Sharma,William Santiago, and Norman McCulloch; ADVANCES IN WOUND CARE, VOLUME 6, NUMBER 6
- Seizure incidence by treatment pressure in patients undergoing hyperbaric oxygen treatment; Marvin Heyboer III, Shane Jennings, William D. Grant, Cindy Ojevwe, Joseph Byrne, Susan M. Wojcik; UHM 2014, Vol. 41, No. 5
- Oxygen toxicity seizures: 20 years' experience from a single hyperbaric unit; Neil D G Branham; Diving and Hyperbaric Medicine, Vol 41, No. 4, December 2011
Is there any sort of consensus on how to alter a treatment protocol such as increased number of air breaks or treatment depth?
A: No. Practically speaking one may decreased depth, decrease length, and add air breaks. No study has demonstrated efficacy, but it makes theoretical sense.
Are there thresholds to clear to treat such as length of time to be seizure-free (on or off antiseizure meds)?
A: No. Recommendation is stable on anti-seizure medication. Epilepsy has never been identified as an actual risk factor although theoretical risk.
Or is such a patient at the same risk as any other patient?
A: Literature says same risk, but not unreasonable during informed consent to acknowledge possible increased risk.
There is no formula for adjusting a dive profile to decrease the likelihood of having a seizure. Likewise, there is no model, formula or nomogram that forecasts the likelihood of an oxygen induced seizure when patient presents with a history of seizure disorder. The important thing is to make sure that the patient’s seizure medications are appropriately dosed and taken by the patient. Blood levels if available should be obtained. We assume that O2 induced seizures are more likely when patients with an underlying seizure disorder (or fever) is present but even that assumption is mostly an educated guess.
In terms of adjusting the profile, of course it depends on the pressure you are using for treatment and what the disorder being treated is. If it is a 2.4 ATA profile I would begin increasing the frequency of air breaks to every 20 minutes for a 5 minute duration. If a seizure occurs there, I would reduce the pressure to 2.0 ATA and continue air breaks (probably every 30 minutes). I would avoid any futher reduction of pressure if possible.
If it is a 2.0 ATA profile I would introduce air breaks if none are being used. I would begin with 5 minutes every 30 minutes. If a seizure occurs I would introduce the air breaks every 20 minutes for 5 minutes. I would not reduce pressure downward from 2.0 ATA.
If it is a 2.8 or 3.0 ATA profile, I would increase the frequency of air breaks, but a stepwise pressure decrease might be needed as well. Obviously, these treatments would be for a diving case or perhaps a gas gangrene or necrotizing fasciitis. In that case pressures should be maintained if at all possible and the best option is to increase the frequency of air breaks. Care should be taken in ascending to a lower pressure especially in a table VI or other similar profile for DCS so as to not make the DCS or Air Embolism worse.
I hope this provides you with some guidance. In my experience, it is an empirical adjustment. Obviously, you will have selected a particular treatment profile because you thought it was appropriate for that patient. I would avoid radical changes and make only minor adjustments. In my experience, the shortening of O2 periods and increased frequencies of air breaks usually works well.
We have a patient who was initially treated with external beam radiation for prostate cancer. About 5 years later he was found to have a recurrence of this cancer and was treated with Radioactive Beads. He now has issues Radiation Cystitis associated with pain and hematuria. However he was found on the last cystoscopy/TURP to have areas of necrotic tumor on his prostate. The Urologist has referred him for HBO therapy for the symptomatic Radiation Cystitis. Are there contraindications for HBO ther
Posted: 12/7/2010
Q:
We have a patient who was initially treated with external beam radiation for prostate cancer. About 5 years later he was found to have a recurrence of this cancer and was treated with Radioactive Beads. He now has issues Radiation Cystitis associated with pain and hematuria. However he was found on the last cystoscopy/TURP to have areas of necrotic tumor on his prostate. The Urologist has referred him for HBO therapy for the symptomatic Radiation Cystitis. Are there contraindications for HBO therapy for the Radiation Cystitis, while he apparently may have ongoing active Prostate Cancer.
A:
One of the topics that has come up in our center is the concern surrounding treating active cancer (CA) patients. I would really appreciate your thoughts on this topic. From all the studies I've read, there still seems to be a fair amount of ambiguity in this area. Above all, I've yet to read a study where the results are conclusive; whether for or against the usage of HBO2 for the treatment of CA. As a medical director, how do you approach these patients during the initial consultation with regards to the medical legal aspect?
I am attaching the paper I did a number of yrs ago which was fairly comprehensive at that time. Since then there have been a smattering of papers, mostly case reports or pre-clinical studies which are a mixed bag. I am still convinced that the evidence supporting a renewal or acceleration of cancer growth is not at all impressive. I advise those who ask me to include a statement like this in their consent..."While the vast majority of published papers show no evidence of cancer recurrence or enhanced growth, based on a few papers with very few patients some authors have expressed their concerns about cancer growth. You should take this information under consideration if you decide to have hyperbaric treatments." Many publications that question the issue of cancer growth and suggest that HBO does enhance growth are directly contradicted by papers of the same or similar design
See attached. It is not a straightforward issue. Some patients with cancer recur and some develop rapid growth (probably after collapse of their inherent immune response.) This happens whether or not they have HBO treatments.”
The paper you attached is https://www.uhms.org/images/MEDFAQs/October-21-2016/Feldmeier_HBO_and_Malignancy.pdf
Also see the additional papers below:
- Hyperbaric Oxygen Therapy for Malignancy: A Review; Jurstine Daruwalla, B.Sc, Chris Christophi, MD; World J Surg (2006) 30: 2112–2131
- Hyperbaric Oxygen: Does it promote growth or recurrence of malignancy?; J. Feldmeier, U. Carl, K. Hartmann, P. Sminia; UHM 2003, Vol. 30, No. 1
- Hyperbaric oxygen therapy and cancer—a review; Ingrid Moen & Linda E. B. Stuhr; Targ Oncol (2012) 7:233–242
If a patient with a Wagner Grade 3 ulcer has osteomyelitis that has failed all conservative measurement is being worked up for HBO. He continues to work as a EMT and does 24 hour shifts twice a week, including weekdays and can only commit to HBO three days a week. Would this be acceptable therapy for the chronic osteomyelitis, or would this be considered inappropriate if the therapy is not done five days a week. I don't want the commercial insurance company coming back and requesting their payment bac
Postd: 12/7/2020
Q:
A patient with a Wagner Grade 3 ulcer has osteomyelitis that has failed all conservative measurement is being worked up for HBO. He continues to work as a EMT and does 24 hour shifts twice a week, including weekdays and can only commit to HBO three days a week. Would this be acceptable therapy for the chronic osteomyelitis, or would this be considered inappropriate if the therapy is not done five days a week. I don't want the commercial insurance company coming back and requesting their payment back.
A:
The standard treatment with HBO2 is 5 treatments per week for chronic osteo or for Wagner’s 3 diabetic foot ulcers. We don’t know whether a course of treatment with substantially fewer than 5 treatments per week will be effective. This has never been studied. Another issue of course is while he is working as an EMT he is likely on his feet for a good portion of the time making offloading very difficult. We can’t predict what the insurance company will do. You might think of a course of HBO2 on a 3 times a week basis or some other less than 5 treatment per week course as being analogous to taking an antibiotic only for a few days each week. It is very unlikely to be successful. I would try to prevail upon the patient to take a leave of absence (hopefully with some kind of pay) to address his problem with a multi-disciplinary treatment including aggressive antibiotics, HBO2, appropriate surgical debridement and adequate offloading.
John J. Feldmeier, D.O.
I have a patient with severe Crohn's disease and multiple abdominal wall fistulas that has been told she is not a surgical candidate. She is already on TPN with limited liquid PO. Does anyone have advice for treatment protocols, length of course, things to look out for, etc.?
Posted: 12/7/2020
Q:
I have a patient with severe Crohn's disease and multiple abdominal wall fistulas that has been told she is not a surgical candidate. She is already on TPN with limited liquid PO. Does anyone have advice for treatment protocols, length of course, things to look out for, etc.?
A:
There are numerous small case series reporting the results of hyperbaric oxygen in the treatment of inflammatory bowel disease (Crohns and Ulcerative Colitis). Typically these are positive in results for a majority of cases often including patients refractory to pharmacologic treatment and in Crohns including patients with fistulae.
Below is a review article that summarizes much of the literature and gives details on treatment protocols used. Toxicities have been very rare and generally the typical side effects encountered in the clinical practice of hyperbaric oxygen.
Hyperbaric oxygen treatment for inflammatory bowel disease: a systematic review and analysis; Daniel A Rossignol; Rossignol Medical Gas Research 2012, 2:6
i have a pt that we are working up for HBO. He has a significant psych history, including schizophrenia. He is taking quetiapine citalopram, and trazodone. Will these medications have a safe interaction with the high concentration of oxygen?
Posted: 12/7/2020
Q:
I have a pt that we are working up for HBO. He has a significant psych history, including schizophrenia. He is taking quetiapine citalopram, and trazodone. Will these medications have a safe interaction with the high concentration of oxygen?
A:
There are no specific published experiences of these three agents. In the latest version of the Kindwall textbook, Hyperbaric Medicine Practice. Dr. Ryan Feldman in his article in the Kindwall textbook (page 149, 4th Edition) discusses the issue of psychotopics and HBO2. One mechanism for their effects is the increase of serotonin levels in the CNS in the synaptic space by interfering with cellular reuptake. The chapter in the Kindwall textbook discusses chloropromazine and prochlorpromazine specifically and notes that have been reported to reduce oxygen toxicity.
In regard to the drugs you are inquiring about, I have the following remarks:
Quietapine (Seraquel)also works through serotonin receptors. Quietapine’s side effects include low blood pressure with standing, seizures, a prolonged erection, high blood sugar, tardive dyskinesia, and neuroleptic malignant syndrome.
Theoretically, a patient receiving HBO2 and this drug might have a lower threshold for seizure onset. Consideration should be given to alteration in the HBO2 treatment profile to decrease the likelihood of seizures.
Citalopram (Celexa): It is an SSIR (Selective Serotonin Reuptake Inhibitors)like Quietadine.
Listed below are conditions that patients are advised to discuss with their physicians before starting Citalopram.
- a bleeding or blood clotting disorder;
- liver or kidney disease;
- narrow-angle glaucoma;
- seizures or epilepsy;
- heart disease, heart failure, a heart rhythm disorder, slow heartbeats, or recent history of heart attack;
- personal or family history of Long QT syndrome;
- an electrolyte imbalance (such as low levels of potassium or magnesium in your blood);
- bipolar disorder (manic depression); or
- a history of drug abuse or suicidal thoughts.
To me the list implies a likely increase of risk for seizure as above for Quietapine. As above the patient should be carefully observed for any prodromes of a seizure while in the chamber and consideration could be given to altering the HBO2 protocol to reduce the risk of seizure.
Trazadone
At higher dose Trazadone also can act as an SSIR.
Its list of more common cautions for Trazadone include:
- Bipolar disorder
- Kidney or liver disease
- Blood or bleeding disorders
- Heart disease
- A heart rhythm problem called long QT syndrome
- Low blood pressure
- Low blood sodium
- Recent heart attack
No indication that I could find indicated that it too presented a risk for seizures.
In terms of how to put this all together, we can only say that psychotropics have been used with HBO2 before without significant complications. Trazadone and Celexa are common drugs and I have to believe that they have been given with HBO2 before and nor reports of negative interaction of these drugs was found on literature search.
Two of the 3 drugs seem to have a risk for seizure. I would probably begin the patient at 2.0 ATA and introduce airbreaks every 30 minutes. If he or she does well, you might then consider increasing pressure or length of O2 treatment.
As always, the decision to treat or not treat is the purview of the hyperbaric physician and our remarks are only meant to provide what information is discoverable.
Is it acceptable to have a Certified Medical Assistant performing hyperbaric treatments? I have heard of it in the past but wasn't sure if it is still acceptable. I do know that they cannot certify anymore unless they have a current EMT status.
Posted: 12/15/2020
Q:
Is it acceptable to have a Certified Medical Assistant performing hyperbaric treatments? I have heard of it in the past but wasn\'t sure if it is still acceptable. I do know that they cannot certify anymore unless they have a current EMT status.
A:
Thank you for your question!
I’ve included the link to the UHMS’s PS on certification - https://www.uhms.org/images/Position-Statements/position_statement_-_uhms_associates_hyperbaric_certification_recognition_v.10.05.2019_v6_1.pdf.
A CMA does qualify as a qualifying pathway for the ABWH’s CWS exam and certification but not for the NBDHMT’s CHT. Those links are listed below.
https://abwh.net/get-certified/certified-hyperbaric-specialist/
https://www.nbdhmt.org/forms/CHT_Resource_Manual.pdf - qualifying pathway page 1
I have a question for management of CRAO patients who are hospitalized for HBOT: This presupposes the patient showed some response to the first dive. Due to staffing limitations, we treat CRAO patients who respond to first treatment (but have not returned to normal vision) on a BID basis until plateau has been reached. I am interested in best evidence to support use of supplemental normobaric oxygen between HBOT. I would be interested in other facilities approach. A related question is how other facilitie
Posted: 12/15/2020
Q:
I have a question for management of CRAO patients who are hospitalized for HBOT: This presupposes the patient showed some response to the first dive. Due to staffing limitations, we treat CRAO patients who respond to first treatment (but have not returned to normal vision) on a BID basis until plateau has been reached. I am interested in best evidence to support use of supplemental normobaric oxygen between HBOT. I would be interested in other facilities approach.
A:
For patient's being treated for CRAO (Central Retinal Artery Occlusion) with BID HBO2, what is the best evidence for dosing and frequency of normobaric supplemental oxygen between HBOT treatments?
This answer is from Dr. Heather Murphy-Lavoie who has published and spoken extensively on this topic:
“The patient should be treated BID at the of return of vision or 2.8ATA if no improvement. Treat until no further improvement for three days or recanalization proven by fluorescein angiogram. Between treatments patients should ideally be admitted to the hospital on a stroke protocol where they can be monitored. Oxygen is given for 15 min every hour only if it is needed to maintain viability of the retina between treatments. The Hyperbaric Oxygen Therapy Indications Manual, 14th Edition has more detail on this subject.”
What is the best approach of treating pediatric patients in monoplace chambers? Is it safe to allow a parent inside the chamber with the child?
12/21/2020
Q:
What is the best approach of treating pediatric patients in monoplace chambers? Is it safe to allow a parent inside the chamber with the child?
A:
Thank you for your question. The UHMS HBO2 Safety Committee can provide information to assist you in answering your question, but the ultimate responsibility for these types of questions rests with the Medical Director and Safety Director of your facility.
The UHMS HBO2 Safety Committee is aware of several facilities that allow this practice, provided that several risk mitigations are in place prior to therapy. While NFPA-99 classifies chambers based on occupancy, Class A (human - multiple occupancy) or Class B (human - single occupancy), the document does not prohibit this practice. The Food and Drug Administration allows the Off-Label Use of Medical Devices under the Supervision of a Physician and subject to certain, safety-based criteria. We suggest applying this principle to the scenario above.
The UHMS HBO2 Safety Committee recommends that the Hyperbaric Medical Director and Hyperbaric Safety Director examine the risks and benefits of this approach with each particular patient and consider the safety mitigations described below before proceeding with this practice. We also recommend that the facility develop standardized procedural guidance for this scenario ahead of time and discuss the approach with the hyperbaric staff. There may be the need to gather information from your legal and administrative teams before engaging in this practice, so we encourage that procedural guidance and equipment needs are ready before the consult is realized.
Please consider the following safety mitigations and recommendations pertaining to the practice of the treatment of a patient with an occupant caregiver in the monoplace chamber:
- We recommend that the occupant caregiver be a parent, guardian or relative that is well known to the patient. If possible, try to maintain consistency with that individual throughout the treatment plan.
- Have a plan in the event that the primary occupant caregiver is unable to be in the chamber, so as not to interrupt the treatment plan for the patient.
- We recommend grounding both the patient and the occupant caregiver, and test the continuity of both devices prior to every therapy.
- An individual breathing apparatus should be available for each occupant where air breaks are used.
- Consider the use of “wye” connections for grounding and air break purposes.
- Ensure that the air break mask is properly suited for the adult/pediatric patient, as applicable.
- The Hyperbaric Physician should provide thorough education to the occupant caregiver and provide instruction on how to respond to the side effects of therapy
- The Hyperbaric Physician should evaluate the occupant caregiver for the risks of hyperbaric oxygen therapy and gain consent as they would a patient.
- The facility should have a plan to respond to an incapacitated occupant caregiver (seizure activity, cardiac arrest, etc.).
- Consider documenting in the occupant caregiver’s chart and treating this as a separate appointment
- Consider a nominal or ‘no-charge’ visit for the occupant caregiver
- Avoid the use of clinical staff as occupant caregivers – the oxygen exposure creates an additional occupational risk and may be a complicated matter from the perspective of occupational health and human resources (job description/job expectations). Consult with these groups before considering this approach.
- Anticipate the need to consult with your hospital’s Administration, Safety Management, and Legal teams. Ensure that any safety, liability, or reimbursement concerns are addressed.
Also noteworthy, the National Board of Diving and Hyperbaric Medical Technology released a statement in 2011 related to this practice:
“…the Board of Directors has posted a new Position Statement (July 2011; 2011-02). It relates to the not uncommon practice of having a pediatric patient accompanied in a monoplace chamber. The decision to require a staff or family member to join such patients is entirely that of the treating hyperbaric physician and presumably a decision based upon a risk-benefit assessment. It is not the intent of this latest Position Statement to argue the relative merits of this practice. Rather, the Board wants to ensure that should dual occupancy occur it does so with relevant safety standards considered.” Link
References:
Optimizing the pediatric hyperbaric oxygen therapy plan: Tandem therapy - Nicholas Marosek, RN, CHRN, UHMS Safety Pre-Course, June 2019
Celebi, A. R. C., Kadayifcilar, S., & Eldem, B. (2015). Hyperbaric oxygen therapy in branch retinal artery occlusion in a 15-year-old boy with methylenetetrahydrofolate reductase mutation. Case reports in ophthalmological medicine, 2015.
Fok, T. F., Shing, M. K., So, L. Y., & Leung, R. K. W. (1990). Vascular Air Embolism‐Possible Survival. Acta Pædiatrica, 79(8‐9), 856-859.
Hsieh, W. S., Yang, P. H., Chao, H. C., & Lai, J. Y. (1999). Neonatal necrotizing fasciitis: a report of three cases and review of the literature. Pediatrics, 103(4), e53-e53.
Korambayil, P. M., Ambookan, P. V., Abraham, S. V., & Ambalakat, A. (2015). A multidisciplinary approach with hyperbaric oxygen therapy improve outcome in snake bite injuries. Toxicology International, 22(1), 104. Liebelt, E. L. (1999).
Hyperbaric oxygen therapy in childhood carbon monoxide poisoning. Current opinion in pediatrics, 11(3), 259-264.
Mader, J. T., Adams, K. R., Wallace, W. R., & Calhoun, J. H. (1990). Hyperbaric oxygen as adjunctive therapy for osteomyelitis. Infectious disease clinics of North America, 4(3), 433-440.
Smith-Slatas, C. L., Bourque, M., & Salazar, J. C. (2006). Clostridium septicum infections in children: a case report and review of the literature. Pediatrics, 117(4), e796-e805.
Tsung, J. W., Chou, K. J., Martinez, C., Tyrrell, J., & Touger, M. (2005). An adolescent scuba diver with 2 episodes of diving-related injuries requiring hyperbaric oxygen recompression therapy: a case report with medical considerations for child and adolescent scuba divers. Pediatric emergency care, 21(10), 681-686.
Waisman, D., Shupak, A., Weisz, G., & Melamed, Y. (1998). Hyperbaric oxygen therapy in the pediatric patient: the experience of the Israel Naval Medical Institute. Pediatrics, 102(5), e53-e53.
Respectfully,
The UHMS HBO2 Safety Committee
DISCLAIMER
Neither the Undersea and Hyperbaric Medical Society (UHMS) staff nor its members are able to provide medical diagnosis or recommend equipment over the internet. If you have medical concerns about hyperbaric medicine you need to be evaluated by a doctor licensed to practice medicine in your locale, which can provide you professional recommendations for hyperbaric medicine based upon your condition. The responsibility of approving the use of equipment resides with the physician and safety director of the facility. Information provided on this forum is for general educational purposes only. It is not intended to replace the advice of your own health care practitioner and you should not rely upon it as though it were specific medical advice given to you personally.
Under UHMS and/or CMS guidelines, can HBO therapy be utilized to support artificial skin grafts? If so, are there any ways which approach to use of HBOT might differ from support of a compromised flap/graft?
Posted: 1/12/2021
Q:
Under UHMS and/or CMS guidelines, can HBO therapy be utilized to support artificial skin grafts? If so, are there any ways which approach to use of HBOT might differ from support of a compromised flap/graft?
A:
These are the ICDs for compromised graft that are approved for treatment with HBO2. By definition, autograft and allograft can’t be artificial.
996.52 Mechanical complication due to graft of other tissue, not elsewhere classified T86.820 Skin graft (allograft) rejection
996.52 Mechanical complication due to graft of other tissue, not elsewhere classified T86.821 Skin graft (allograft) (autograft) failure
996.52 Mechanical complication due to graft of other tissue, not elsewhere classified T86.822 Skin graft (allograft) (autograft) infection
996.52 Mechanical complication due to graft of other tissue, not elsewhere classified T86.828 Other complications of skin graft (allograft) (autograft)
I completed an HBO consult on a patient regarding a wound in an irradiated area. He is currently on cabozantinib regarding metastatic renal cancer. My question is, the mechanism of action of this chemo medication in inhibiting VGEF resulting in decrease angiogenesis. Is this reason not to treat him? Won’t this be going against the benefit of HBO trying to promote angiogenesis? Thank you for any input.
Posted: 2/3/2021
Q:
I completed an HBO consult on a patient regarding a wound in an irradiated area. He is currently on cabozantinib regarding metastatic renal cancer. My question is, the mechanism of action of this chemo medication in inhibiting VGEF resulting in decrease angiogenesis. Is this reason not to treat him? Won’t this be going against the benefit of HBO trying to promote angiogenesis? Thank you for any input.
A:
Cabozantinib and HBO2:
As the writer has pointed out, this drug interferes with VEGFR2 (One of 3 receptors for vascular endothelial growth factor). This receptor is involved in wound healing.
I also agree that using it with hyperbaric oxygen is likely to diminish the effectiveness of HBO2 in promoting angiogenesis as an essential part of wound healing.
Another potential effect is by providing more VEGF activity, the HBO2 may diminish the effectiveness of the drug in its impact on the cancer.
We do not have any published clinical experience with the combination of the 2 modalities. However, based on an understanding of their mechanisms and common sense, I would recommend not giving HBO2 and Cabozantinib concurrently.
It has a fairly long serum half life (120 hours) and has been shown to increase fivefold in concentration over a fifteen day administration.
See abstract below:
Clinical Pharmacokinetics and Pharmacodynamics of Cabozantinib
Steven A Lacy 1, Dale R Miles 2 3, Linh T Nguyen 2 4
Affiliations expand
- PMID: 27734291
Abstract
Cabozantinib inhibits receptor tyrosine kinases involved in tumor angiogenesis and metastasis. The capsule formulation (Cometriq®) is approved for the treatment of progressive metastatic medullary thyroid cancer at a 140-mg free base equivalent dose. The tablet formulation (Cabometyx™, 60-mg free base equivalent dose) is approved for the treatment of renal cell carcinoma following anti-angiogenic therapy. Cabozantinib displays a long terminal plasma half-life (~120 h) and accumulates ~fivefold by day 15 following daily dosing based on area under the plasma concentration-time curve (AUC). Four identified inactive metabolites constitute >65 % of total cabozantinib-related AUC following a single 140-mg free base equivalent dose. Cabozantinib AUC was increased by 63-81 % or 7-30 % in subjects with mild/moderate hepatic or renal impairment, respectively; by 34-38 % with concomitant cytochrome P450 3A4 inhibitor ketoconazole; and by 57 % following a high-fat meal. Cabozantinib AUC was decreased by 76-77 % with concomitant cytochrome P450 3A4 inducer rifampin, and was unaffected following administration of proton pump inhibitor esomeprazole. Cabozantinib is a potent in vitro inhibitor of P-glycoprotein, and multidrug and toxin extrusion transporter 1 and 2-K, and is a substrate for multidrug resistance protein 2. No clinically significant covariates affecting cabozantinib pharmacokinetics were identified in a population pharmacokinetic analysis. Patients with medullary thyroid cancer with low model-predicted apparent clearance were more likely to dose hold/reduce cabozantinib early, and had a lower average dose through day 85. However, longitudinal tumor modeling suggests that cabozantinib dose reductions from 140 to 60 mg/day did not markedly reduce tumor growth inhibition in medullary thyroid cancer patients.
Is there any reason/ caution to take in diving an 80 y/o woman s/p resection of left jaw and tongue for SCC 1982- post radiation. During her resection the vagus phrenic nerve was cut resulting in paralysis of her left diaphragm. I spoke with her pulmonologist. He states she has 47% lung capacity, mild asthma and OSA. He states he knows nothing about HBO and cannot say whether she would be safe diving or not. She runs an 88-94% O2 on room air. She is not on supplemental O2 and is asymptomatic- no SOB. The
Posted: 2/12/2021
Q:
Is there any reason/ caution to take in diving an 80 y/o woman s/p resection of left jaw and tongue for SCC 1982- post radiation. During her resection the vagus phrenic nerve was cut resulting in paralysis of her left diaphragm. I spoke with her pulmonologist. He states she has 47% lung capacity, mild asthma and OSA. He states he knows nothing about HBO and cannot say whether she would be safe diving or not. She runs an 88-94% O2 on room air. She is not on supplemental O2 and is asymptomatic- no SOB. The plan is to dive her for orn with dental caries and dry mouth- in need of dental extraction with pre/post HBOT @ 2.5ATA w/ 2 air breaks x 20 up front and 10 after tx.
A:
From a safety point of view, assuming she doesn’t have bullous disease she should be fine with HBO2 unless she is a CO2 retainer (baseline hypercapnia). If her PCO2 is significantly elevated (i.e. greater than 48 mmHg) she may become more hypercapnic in the chamber, which would predispose her to CNS O2 toxicity.
However, with her baseline hypoxemia it is possible she may not achieve a therapeutic PO2 during hyperbaric therapy. If her asthma is under good control I suggest obtaining a baseline ABG on room air, from which her PO2 during HBO2 could be estimated.
We currently have a patient with RTI to head and neck. She had HBO in 2011 and 2012 for ORN of the mandible. She is now having an extraction of a tooth and surgeon is ordering 10 HBO post extraction. We follow the protocol of 20/10 HBO as stated in our LCD in Penna.from 2019. Many years ago we followed a protocol of 10 HBO post extraction if patient had HBO within 5 years of new extraction. This patient is 9 years post HBO. What is the protocol that we should be using? We do not have a new LCD to follow.
Posted: 2/19/2021
Q:
We currently have a patient with RTI to head and neck. She had HBO in 2011 and 2012 for ORN of the mandible. She is now having an extraction of a tooth and surgeon is ordering 10 HBO post extraction. We follow the protocol of 20/10 HBO as stated in our LCD in Penna.from 2019. Many years ago we followed a protocol of 10 HBO post extraction if patient had HBO within 5 years of new extraction. This patient is 9 years post HBO. What is the protocol that we should be using? We do not have a new LCD to follow. The doctor is questioning the 20 treatments pre extraction.
A:
Dr. Marx who designed the protocols believes, based on transcutaneous measurements he has done on a group of patients 2 and even 3 yrs out from HBO2, that improvement in the radiation damaged vascularity is permanent. He saw no regression in levels obtained immediately after completion of the HBO2 when compared to the 2 and 3 yr. measurements.. He does not recommend pre-extraction HBO for a patient like yours who has had 2 prior course of HBO2. The 10 post-extraction HBO2 treatments are prudent in my judgement. If the patient were to have delayed healing with exposed bone after these ten, consideration to perhaps an additional 10 to 20 treatments could also be considered. If healing after the 10 post-extraction is progressing nicely, no additional treatments will be needed.
We currently have a patient with RTI to head and neck. She had HBO in 2011 and 2012 for ORN of the mandible. She is now having an extraction of a tooth and surgeon is ordering 10 HBO post extraction. We follow the protocol of 20/10 HBO as stated in our LCD in Penna.from 2019. Many years ago we followed a protocol of 10 HBO post extraction if patient had HBO within 5 years of new extraction. This patient is 9 years post HBO. What is the protocol that we should be using? We do not have a new LCD to follow.
Posted: 2/22/2021
Q:
We currently have a patient with RTI to head and neck. She had HBO in 2011 and 2012 for ORN of the mandible. She is now having an extraction of a tooth and surgeon is ordering 10 HBO post extraction. We follow the protocol of 20/10 HBO as stated in our LCD in Penna.from 2019. Many years ago we followed a protocol of 10 HBO post extraction if patient had HBO within 5 years of new extraction. This patient is 9 years post HBO. What is the protocol that we should be using? We do not have a new LCD to follow.
A:
Dr. Marx who designed the protocols believes, based on transcutaneous measurements he has done on a group of patients 2 and even 3 yrs. out from HBO2, that improvement in the radiation damaged vascularity is permanent. He saw no regression in levels obtained immediately after completion of the HBO2 when compared to the 2 and 3 yr. measurements post HBO2. He does not recommend pre-extraction HBO2 for patients who have had 2 prior courses or even 1 prior course of HBO2 with either the 20/10 in association with extractions or a 30/10 course for the treatment of existent ORN. The 10 post-extraction HBO2 treatments are prudent in my judgement. If the patient were to have delayed healing with exposed bone after these ten, consideration to perhaps an additional 10 to 20 treatments could also be considered. If healing after the 10 post-extraction is progressing nicely, no additional treatments will be needed. If the oral surgeon finds more ORN at the time of the extractions, consideration should be given to a full forty treatments to treat recurrent ORN
I have a 45 y.o. M with hx of R sudden hearing loss and hx of posterior fossa approach for brain tumor removal, and still has a right posterior ventriculoperitoneal catheter. He needs hyperbaric tx for sudden hearing loss of now L ear. Is it safe to dive a patient with VP cathether
Posted: 3/2/2021
Q:
I have a 45 y.o. M with hx of R sudden hearing loss and hx of posterior fossa approach for brain tumor removal, and still has a right posterior ventriculoperitoneal catheter. He needs hyperbaric tx for sudden hearing loss of now L ear. Is it safe to dive a patient with VP catheter?
A:
Thank you for your question. The UHMS HBO2 Safety Committee can provide information to assist you in answering your question, but the ultimate responsibility for these types of questions rests with the Medical Director and Safety Director of your facility.
For the sake of the reader who may not be familiar with this device, a ventriculoperitoneal catheter (or shunt) is used to drain excess cerebrospinal fluid (CSF) from the brain. The shunt works by moving fluid out of the brain by way of a one-way valve with reservoir connected to a short and long catheter routed to the abdomen where the fluid can be absorbed. This lowers the pressure and swelling on the brain.
The UHMS HBO2 Safety Committee observes that this device is fluid-filled and should behave similarly compared with other fluid lines and drains that are consistently allowed in chambers. One concern may be the lack of access and fluid control that the provider may have to the patient if therapy is provided in a monoplace chamber. We recommend that these and all other risks to the patient are identified in a risk assessment performed by the Safety Director and Medical Director of your facility. We also recommend reaching out to the device manufacturer, as there are programmable versions of these shunts with greater complexity.
There is at least one published article describing a successful test of a VP shunt under Hyperbaric conditions, “Ventriculo-peritoneal shunt performance under hyperbaric conditions.” The Safety Committee reached out to one of the authors of this article, who stated: “This testing was performed on a specific Medtronic VP shunt. Theoretically if the shunt is all fluid filled and had no mechanical parts, it should function as intended under hyperbaric conditions. We did the testing just to confirm that it did, but I would recommend that whomever is treating the patient should go through the same thought process (not necessarily the testing) as they would to evaluate any equipment that is to go in the chamber.”
Other considerations and observations from the UHMS HBO2 Safety Committee include:
- I have treated a few patients with these over the years. I have approached their approval-to-dive as I would for any other fluid filled and fully implanted device.
- Think of the VP shunt like a siphon. It is fluid filled, so generally there no worries with HBOT unless this shunt is in an inside attendant. There is an underlying reason (usually hydrocephalus) that would make me think twice about subjecting an employee to pressure routinely.
- There might be an extra consideration depending on how the back-check valve operates for a given device, but I’ve only seen ones that open based on elevated ICP and not any biomechanical process that universally applied pressure or oxygen gradients would affect. Still always double check with the manufacturer every time, though.
- We have treated numerous patients with a VP shunt and as the shunt is fluid filled it has not been an issue.
- We have routinely allowed patients with the older non-programmable shunts to go into the chamber. We also let the newer programmable devices in. However, the last time we checked they were not formally pressure tested by the manufacturer. The manufacturer did have reports of their shunts in the HBO environment without issue. I haven’t contacted the company of late.
Respectfully,
The UHMS HBO2 Safety Committee
REFERENCES:
Burman, F. (2019). “Risk Assessment Guide for Installation and Operation of Clinical Hyperbaric Facilities,” (6th ed.). San Antonio, TX: International ATMO, Inc.
Huang ET, Hardy KR, Stubbs JM, Lowe RA, Thom SR. “Ventriculo-peritoneal shunt performance under hyperbaric conditions.” Undersea Hyperb Med. 2000 Winter; 27(4):191-4. https://pubmed.ncbi.nlm.nih.gov/11419359/
Memorial Sloan Kettering Cancer Center, “About Your Ventriculoperitoneal (VP) Shunt Surgery.” Accessed 02/26/2021. https://www.mskcc.org/cancer-care/patient-education/about-your-ventriculoperitoneal-vp-shunt-surgery
DISCLAIMER
I recently saw a 52-year-old male with a hx of anaplastic oligodendroglioma, referred by his neuro-oncologist for possible hyperbaric oxygen therapy treatments for brain radiation necrosis and worsening cognitive impairments. In April 2019, the patient had a left craniotomy for removal of a large frontal tumor with hemorrhage and herniation with pathology of anaplastic oligodendroglioma WHO grade 3. He had radiation therapy (5940 cGy) July-August 2019 and concurrent TMZ (Temozolomide) chemotherapy. A
Posted: 5/17/2021
Q:
I recently saw a 52-year-old male with a hx of anaplastic oligodendroglioma, referred by his neuro-oncologist for possible hyperbaric oxygen therapy treatments for brain radiation necrosis and worsening cognitive impairments. In April 2019, the patient had a left craniotomy for removal of a large frontal tumor with hemorrhage and herniation with pathology of anaplastic oligodendroglioma WHO grade 3. He had radiation therapy (5940 cGy) July-August 2019 and concurrent TMZ (Temozolomide) chemotherapy. After a stereotactic brain biopsy of lesion in left splenium of the corpus callosum in November 2020, he was placed on Bevacizumab for radiation necrosis.
Patient had a stereotactic left-brain biopsy in early May 2021 for a worsening corpus callosum lesion. Pathology report: necrotic brain parenchyma with rare intermixed atypical cells, suspicious for tumor.
The next day, the pathology report shows “ …. This confirms that he does have a recurrence of oligodendroglioma, as the cause of the enlarging lesion. There is also a significant element of necrosis present, with diffuse (not nodular/necrotic) tumor.”
Patient is on a nine-day dexamethasone taper to see if it will help improve his cognition, and the patient is about to start chemotherapy: PCV (procarbazine/CCNU/vincristine) with a port being placed for the vincristine.
I am reluctant to treat the radiation necrosis while he is undergoing active cancer therapy.
I would like to get your thoughts about this situation.
A:
These cases are always difficult because there are so many chemo agents now including targeted therapies. biologics and immune enhancing agent.
If the patient has had Bevacizumab in the past 4 months, I would not treat him with HBO. The drug is an angiogenesis inhibitor, specifically VEGF. As we know HBO works at least in part by inducing angiogenesis as one of the major growth factors. Intuitively, applying both simultaneously would have you working against yourself. Supposedly, it gives some palliation of brain necrosis by stabilizing vascular integrity and preventing or at least ameliorating interstitial edema.
The new drugs are all well-known and have been around for a while. Procarbazine is an alkylating agent. It works to inhibit DNA, RNA and protein synthesis. CCNU is also known as Lomustine. It is also an alkylator. It is known to lipid soluble and for this reason has better penetration into the brain than many other chemo agents. Vincrisine is in a class of drugs called vinca alkaloids. It inhibits microtubule formation within the cell to prevent successful mitosis. Since this patient has likely combination of tumor necrosis and persistent tumor, it makes your decision even more difficult. One of the characteristics of high-grade brain tumors is necrosis. It is possible to my reading that his problems are all due to tumor. I predict his symptoms will get worse as they taper the decadron.
With HBO2 effects on reducing edema, you may get some near immediate improvement in his brain function. With a persistent or recurrent high-grade tumor his survival is probably measured in less than 6 months. From my investigations, I have found no evidence that you will cause the tumor to be more aggressive. It is going to be aggressive whether you give him HBO2 or not. In terms of the chemo complications being worse with concurrent HBO2, it is impossible to say. Alkylators are said to be radiomimetic. In other words, they cause breaks in DNA strands mediated through free radicals. You may actually provide some sensitization of the tumor to the chemotherapy in the same fashion O2 sensitizes tumors to radiation damage.
I would wait until they have completed their taper of steroids in any case. I expect they will have to return him to the steroids. As sad as it is there is little we can do for this patient and it may be time to pull the plug on therapies.
I have a patient referred to me for treatment of soft tissue radionecrosis of oral mucosa of rt posterior maxilla and posterior rt mandible. Patient has undergone radiation and chemotherapy for carcinoma rt tonsillar fossa and tongue. He is cancer free but has ulceration in treated areas. Oncology has biopsied these areas and no recurrences. Do I have to wait 6 months from therapy to start treatment?
Posted: 7/12/2021
Q:
I have a patient referred to me for treatment of soft tissue radionecrosis of oral mucosa of rt posterior maxilla and posterior rt mandible. Patient has undergone radiation and chemotherapy for carcinoma rt tonsillar fossa and tongue. He is cancer free but has ulceration in treated areas. Oncology has biopsied these areas and no recurrences. Do I have to wait 6 months from therapy to start treatment?
A:
You do not mention how long ago the radiation and chemotherapy were completed or how extensive or deep the ulcerations are.
Also if these ulcerations are at the site of the tumor, it may take a period of time for the body to replace this site with normal tissues after the cancer has been eradicated.
If this is indeed radiation necrosis of the soft tissue, I know of no constraints or prohibition in initiating hyperbaric oxygen. Generally, these types of lesions are painful and interfere with eating. Hyperbaric oxygen should hasten their resolution. You may want to contact the insurance carrier ahead of time and explain the case to guarantee appropriate reimbursement.
EARLY HYPERBARIC OXYGEN THERAPY FOR REDUCING RADIOTHERAPY SIDE EFFECTS: EARLY RESULTS OF A RANDOMIZED TRIAL IN OROPHARYNGEAL AND
NASOPHARYNGEAL CANCER;
Int. J. Radiation Oncology Biol. Phys., Vol. 75, No. 3, pp. 711–716, 200
I have a 40 y/o patient with a large open lower leg wound (lower thigh/popliteal fossa) with an underlying diagnosis of mycoses fungoides. He has had radiation therapy on three separate occasions since 2016 with total dose of 7000cGy, however each treatment episode was not more than 3000cgy. Recent wound biopsies still show tumor. His family is pushing for HBO to try to heal the wound, as his oncology team is reluctant to consider stem cell transplant until the wound is healed. I have 2 questions: 1)
Posted: 2/8/2022
Q:
I have a 40 y/o patient with a large open lower leg wound (lower thigh/popliteal fossa) with an underlying diagnosis of mycoses fungoides. He has had radiation therapy on three separate occasions since 2016 with total dose of 7000cGy, however each treatment episode was not more than 3000cgy. Recent wound biopsies still show tumor. His family is pushing for HBO to try to heal the wound, as his oncology team is reluctant to consider stem cell transplant until the wound is healed. I have 2 questions: 1) his only current treatment for the tumor is Bexarotene (he has failed treatment with multiple other chemotherapy agents) and I can\'t find much info on this. Is it safe in conjunction with HBO? Does it affect wound healing? 2) In terms of possible contribution of prior radiation to poor healing, can I consider this is a possibility even though the total radiation dose was delivered in multiple treatment episodes over more than 5 years?
A:
Background:
Mycosis fungoides (MF) is a primary lymphoma of the skin due to T-Cell lymphocytes. MF is responsible for about 40% of primary skin lymphomas. As an aside T-Cell lymphocytes are responsible for cellular immune response. They directly kill the infecting organism; whereas, B-cell lymphocytes produce antibodies, and it is these antibodies that are the primary effect of B-Cell response and control of infecting organisms. Mycosis fungoides typically presents as a plaque-like, often confluent, sometimes nodular, often erythematous dermatitis. It is often very pruritic. I will attach a photo. It is not typically ulcerative though some of the lesions may demonstrate focal ulcerations. Often times the diagnosis is delayed for years (5-8 years). Survival after diagnosis is 5 to 8 years. Organ involvement is unusual early on but is present in 80% of those who die of their disease.
Oncologic treatment is often dictated by the extent of the disease. If it is localized a local radiation field is often used. If it is generalized, chemotherapies often one of the new targeted or immunologic agents are used. If lymph nodes are involved the prognosis is worse. If there is involvement of internal organs, prognosis is worse yet again. Very early mycosis is often treated with topicals including steroids and some chemo agents. Sometimes a technique of whole-body electron treatment is done for diffuse skin involvement. Ultraviolet light has been used with response in early cases in a technique termed PUVA which uses type A ultraviolet light. More recently systemic agents are used for diffuse involvement. These agents are not typically traditional cytotoxic chemotherapy but are targeted or immune therapies. Drugs used include the monoclonal antibodies Brentuximab and Mogamulizumab. Interferon has also been used for treatment as a modulator of immune response. By the way, Bexatrone is a retinoic acid (Vitamin A). it induces cell differentiation and apoptosis and prevents the development of drug resistance. Note: It also has anti-angiogenic effects and inhibits cancer metastasis. There is some experience with high dose chemotherapy and stem cell transplant but this experience is somewhat limited. Really. In almost all cases curative treatment is not possible but the course of the disease is typically long and theoretically at least it can be prolonged with intervention.
Image of Mycosis Fungoides (pdf)
Your Case:
In general, skin lesions that have tumor in them will not heal. This experience has been seen in primary skin cancers (basal and squamous cells) and lymph nodes with metastatic disease that ulcerate through the skin.
You note that the patient has had 3 prior courses of radiation with a total dose of 7000 cGy and wonder about the time interval between treatment courses and whether late radiation effects are likely to occur. Some in the radiation community believe that the radiated tissues will with time between treatment courses recover radiation tolerance. In my experience, that is certainly not always true and the late effects of the separate courses are additive. Also often, MF patients are treated with treatment fractional doses at 300 or even 500 cGy. These higher than the normal daily dose of 180 to 200 cGy are in fact more damaging for a given total dose. Therefore, I believe that this could well in part be late radiation damage.
I believe offering the patient hyperbaric oxygen is a reasonable option. A trial of therapy for perhaps 20 daily treatments is advised. If the patient is not showing expected response at that point, I believe that the presence of tumor in the lesion is the culprit. Of course the reason that transplant is being held is that the conditioning high dose chemotherapy would be very immunosuppressive and put the patient at risk for cellulitis perhaps advancing to sepsis. It is also possible that the anti-angiogenic effects of Bexatrone will work against the HBO2.
By the way, please let us know how the patient does. It will increase our knowledge. A positive outcome would make a good case presentation because of the rarity of the clinical challenges you face.
I have a 62 y/o patient with radiation cystitis who has already received a total of 80 HBO treatments over the course of 10 months (March 2020-December 2020) for recurrent hematuria. He recently had another episode of hematuria that was treated with clot irrigation only (no cautery needed). He was referred back to me by his urologist. Is there any utility to additional treatment with HBO, given that he has already had 80 treatments within the last 2 years? I realize this is technically a new episode o
Posted: 2/8/2022
Q:
Would it be likely effective to offer more HBO2 to an 62 y/o patient who has already completed 80 HBO2 treatments over 10 months (March-December 2020) for recurrent hematuria?
A:
A few additional bits of information would be helpful. Apparently, the patient had a cessation of hematuria for a at least a short time in December 2020. When did the patient have recurrence of hematuria? What type of tumor did the patient have? Do you have any information on radiation dose or technique-specifically was there an implant or was IMRT the treatment technique? Has the patient required transfusion? Is the patient getting chemotherapy for residual or recurrent tumor?
I share your concerns that it is probably unlikely that additional hyperbaric treatments at this point will be effective. However, I have personal experience with radiation cystitis patients who had durable response after up to 100 treatments. I have also seen patients respond to a second course of treatment after a resolution followed by recurrence.
I would recommend that the patient have a cystoscopy at this time. If the site of hematuria is focal, a local intervention with chemical or electrocautery should be considered. If it is diffuse, the instillation of formalin should be considered. If these are not appropriate or possible and the patient is willing, though unusual, additional Hyperbaric oxygen is a reasonable option. As always, especially, if the tumor was a bladder cancer to begin with, recurrent cancer should be ruled out.
A woman called to ask whether we treated post covid-19 symptoms. She has had many issues including severe fatigue, brain fog, difficulty sleeping and states that she is desperate. She is apparently part of a support group; several people have evidently benefitted from HBOT. Does anyone have any experience treating these folks? The patient is willing to pay out of pocket, but I wonder if there are any institutions with ongoing research studies. We are a small monoplace operation without any capability of d
Posted: 2/14/22
Q:
A woman called to ask whether we treated post covid-19 symptoms. She has had many issues including severe fatigue, brain fog, difficulty sleeping and states that she is desperate. She is apparently part of a support group; several people have evidently benefitted from HBOT. Does anyone have any experience treating these folks? The patient is willing to pay out of pocket, but I wonder if there are any institutions with ongoing research studies. We are a small monoplace operation without any capability of doing controlled studies. Any thoughts would be appreciated. Thank you.
A:
There is no central registry of hyperbaric centers that are treating patients for the persistent symptoms of COVID-19 (the so called “Long Haulers”). Through the “Grapevine” we have heard that several centers are treating these patients. The treatment pressures have varied from less than 2.0 ATA to 2.8 ATA and treatment times of 60 to 90 minutes. Typically, the number of treatments has ranged from 5 to 20 in number.
There are 2 clinical trials registered on the NIH site, clinicaltrials.gov, that are conducting studies of HBO2 for Long Haulers. One from Israel with Dr. Efrati as lead investigator and listed on this website as completed, but no results are available yet. A second study by the Karolinska Institute from Stockholm, Sweden is listed as ongoing. The lead investigator is not given on the website. No co-investigating researchers or institutions in the U.S. are mentioned on the website. On an earlier study, Dr. Pieter Lindholm at the University of California, San Diego had been listed as a co-investigator, and he may have additional information. Otherwise, we would advise that the patient in question make contact with hyperbaric facilities near her home to determine if any are doing such treatments for this patient group. Since many hyperbaric centers have popped up recently that are not treating approved indications and have inadequate medical supervision and resulting safety concerns, we recommend that she determine whether the centers she contacts are treating only approved indications or on clinical trials. A good indicator for the quality of a center’s practice is to determine whether they are treating only approved indications or patients on studies with an occasional treatment outside this guidance for compassionate purposes. We recommend she inquire as to whether the center and its staff are members of the UHMS (Undersea and Hyperbaric Medical Society) or at least follow the recommendations of the UHMS. This recommendation is made because the Society has established high standards for the practice of Hyperbaric Medicine which can be dangerous if not properly delivered. Another good indicator of the quality and safety of the delivery of hyperbaric oxygen is to ensure that a licensed physician is always present during the treatment.
The Society cannot make a broad recommendation advocating hyperbaric oxygen for COVID long haul patients. We recognize that there are physiologic effects of Hyperbaric Oxygen which may be helpful in the treatment of COVID-19. Also, we are aware of unpublished reports that hyperbaric oxygen seems to have been successful in the treatment of some symptoms that persist after the acute infection. We do encourage participation in clinical trials whenever possible. We anxiously await the results of the pending clinical trials. We also recognize that the treating physician is ultimately the decision maker when it comes down to recommending and offering hyperbaric oxygen for a given health problem. As always, he or she needs to consider the potential benefits versus the possible side effects or complications of the therapy.
should HBOT treatment be added to debridement and IV antibiotics for soft tissue clostridium infection
Posted: 5/20/22
Q:
Should HBO2 treatment be added to debridement and IV antibiotics for soft tissue clostridium infection?
A:
Hyperbaric oxygen has been a mainstay in the treatment of Clostridial necrotizing soft tissue infections since the pioneering work of Brummelkamp in Holland in the 1960’s. This work was done along with much of the early work that established hyperbaric oxygen as an appropriate adjunctive treatment for several disorders that we continue to treat. The initial rationale was Clostridial organisms are anerobic bacteria and would likely find hyperbaric oxygen lethal or at least bacteriostatic.
Liquefactive soft tissue necrotizing infections can be caused by several Clostridial species including C. perfringens (the most common) along with C. oedematiens, C. septicum, C. histolyticum, C. bifermentans, and C. fallax. More recent investigation of the Clostridial species causing gas gangrene have shown that they are not strict anerobes. Clostridial perfringens will grow freely in oxygen tensions as high as 30mmHg with some growth even up to tissue oxygen tensions of 70mmHg.
The clostridial organisms release at least 20 toxins which are largely responsible for the lethality and toxicity of the disease. The most studied and most important of these is called alpha toxin. This toxin is responsible in large part for the rapidly spreading liquefactive necrosis which is a prominent feature of the serious infections we know as gas gangrene with the local necrotizing process advancing more than one inch every hour. This toxin also plays a large part in causing systemic toxicities.
Four distinct levels of severity have been described. These include: 1) Diffuse clostridial necrosis with systemic toxicity (true gas gangrene); 2) Localized Clostridial myonecrosis; 3) Clostridial cellulitis with systemic toxicity; and Clostridial cellulitis without toxicity.
Clinical signs of gas gangrene include a mild fever (100 to 101 degrees), a tachycardia of 150 beats per minute or higher which is disproportionately elevated for the fever, and a peculiar sort of sensorium where the patient is intellectually aware of the seriousness of their infection but is emotionally unconcerned, also called “la belle indifference.” Interstitial gas is often shown on radiographic studies. Clinically crepitus may be palpated.
Hyperbaric oxygen should be part of a combined modality therapy including high dose antibiotics and surgical debridement. Hyperbaric oxygen is very useful in helping to distinguish between permanently destroyed damage versus salvageable tissues. We recommend against amputation immediately unless the limb is absolutely and certainly beyond salvage and instead recommend hyperbaric oxygen be initiated prior to any radical surgeries. The intent here is to identify and save as much viable tissue as possible. Antibiotics typically include penicillin and/or clindamycin.
Early diagnosis is generally made by history along with a gram stain of the wound which will show large gram positive rods.
The spectrum of effects of Clostridial infections includes respiratory, cardiac, renal complications and DIC. Often these patients will require heparin therapy.
The most important effect of hyperbaric oxygen appears to be the shut down of further alpha toxin production if/when tissue oxygen tensions are increased to 250 mmHg or higher. Oxygen tensions of 2000 or more mmHg are cytotoxic but may not be achieved in vivo.
Patients with trauma or pre-existing vasculopathies including diabetes are at higher risk for gas gangrene. A common source for gas gangrene is a contaminated wound in a patient with impaired circulation. Gas gangrene can occur post operatively, but compared to trauma this occurrence is relatively rare.
In order to have the best impact of hyperbaric oxygen on the infection as part of the multi-disciplinary management, it is necessary to treat these patient at high pressures and multiple times daily typically for 3 days. Typically 3 treatments are given in the first 24 hours and then BID treatments for the next 2 days. In this writer’s experience, oxygen induced seizures are fairly common because these patients are toxic and treated at high pressures of 3.0 ATA. This usually requires a modification in treatment profile to allow continuation of treatment. Since it is important to achieve high treatment pressures and high tissue oxygen levels in the tissues, it is preferrable to shorten oxygen periods over reducing treatment pressure.
All standard textbooks of hyperbaric oxygen deal present extensive information on the treatment of gas gangrene. The treatment of gas gangrene is one of the 14 indications approved by the UHMS. The Indications Manual 14th Edition is a good reference as well as the Whelan-Kindwall textbook or the Neuman-Thom textbook.
Note: see a typical treatment profile below:
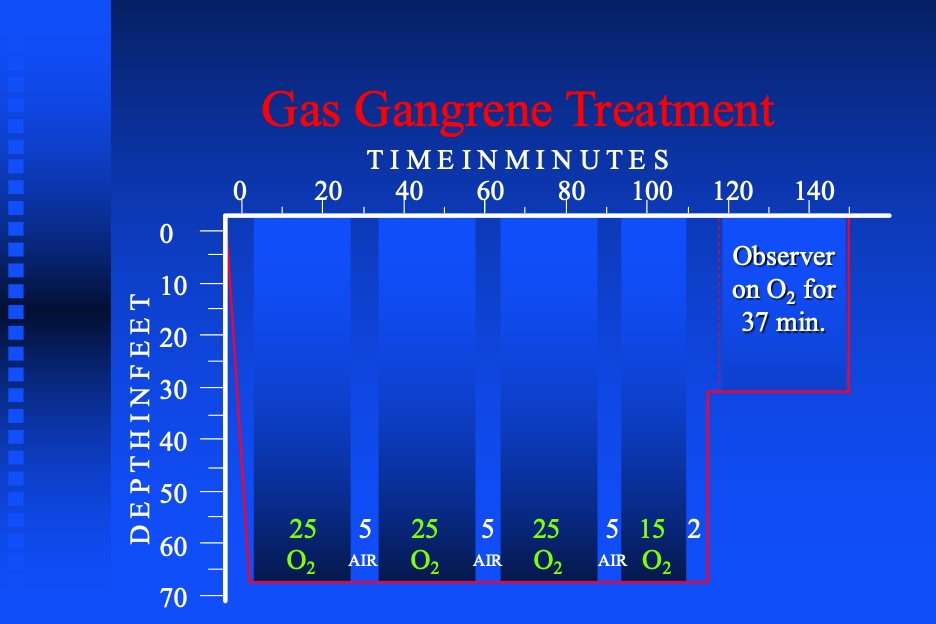
Is hereditary spherocytosis a contraindication to hyperbaric oxygen treatments?
Posted 6/7/22
Q:
Is hereditary spherocytosis a contraindication to hyperbaric oxygen treatments?
A:
Sporadically, there is mention in literature that hyperbaric oxygen may cause increased hemolysis for patients with hereditary spherocytosis. In my search, I was unable to find an original reference citing an organized study or even a case series or case report demonstrating increased hemolysis for spheroid cytosis patients treated with hyperbaric oxygen. I suspect (but cannot prove) that some where along the line, some one speculated that since hyperbaric oxygen causes vasoconstriction that abnormally shaped red blood cells and prone to hemolysis would have more mechanical stress and therefore more hemolysis. Although spherocytosis is relatively rare, I suspect that patients with spheroid cytosis have been previously treated perhaps inadvertently, and we have no reports of increased hemolysis.
I recommend that you include in your informed consent a statement to the effect that some have suggested that there may be increased hemolysis for spheroid cytosis patients undergoing hyperbaric oxygen but that there are reports of patients treated without toxicity. A weekly CBC during treatment would also be prudent, and if there are signs of increased hemolysis, HBO2 should be discontinued and the patient should see his or her hematologist.
Just wondering if the ejection fraction guidelines have changed, we have always followed the greater than 30%, or 25 to 30% if stable, would get cardiac clearance if needed, and what would be considered unstable? clearance if needed, and what would be considered unstable?with cardiac clearance if their
Posted: 10/11/2022
Q:
Just wondering if the ejection fraction guidelines have changed, we have always followed the greater than 30%, or 25 to 30% if stable, would get cardiac clearance if needed, and what would be considered unstable? clearance if needed, and what would be considered unstable?
A:
Re: Left ventricular ejection fraction and hyperbaric oxygen:
This answer originates from Dr. Neil Hampson, M.D who is the retired long term medical director of the Virginia Mason Hyperbaric unit. Dr. Hampson is board certified in Internal Medicine, Pulmonary Medicine, Critical Care and Hyperbaric Medicine. Of course, in addition to the left ventricular ejection fraction, the patient’s recent cardiac history should be obtained and considered. If the patient has recently required medical intervention for cardiac failure issues especially if frequently recurrent, this factor should be included into the decision making in regard to the treatment with hyperbaric oxygen for a non-emergent condition. It is always prudent to consult the patient’s cardiologist when there are concerns about the possibility of inducing congestive heart failure with hyperbaric oxygen treatments.
Here are Dr. Hampson’s recommendations:
Cardiac Screening for HBO2:
- History of cardiac disease – ask to see patient’s last CXR and review last echocardiogram report
- If echocardiogram is greater than one year old and was abnormal, repeat it
- If last echo of any age showed LVEF > 40%, repeat only if cardiac symptoms have progressed since that time
- If echocardiogram performed within one year shows:
- LVEF >30% Proceed with HBO2
- LVEF 20-30% Involve cardiology for optimization prior to considering HBO2
- LVEF <20% No routine HBO2
Radiation cystitis withOUT hematuria: One of our urologists would like to refer patients with incapacitating symptoms of radiation cystitis (frequency, urgency, etc) and evidence of "necrosis" on cystoscopy but no gross hematuria. He has anecdotal evidence that these symptoms improve with HBOT. Is there any support from the literature and /or would cystitis withOUT hematuria be covered by Medicare?
Posted: 5/19/23
Q: Radiation cystitis withOUT hematuria: One of our urologists would like to refer patients with incapacitating symptoms of radiation cystitis (frequency, urgency, etc) and evidence of "necrosis" on cystoscopy but no gross hematuria. He has anecdotal evidence that these symptoms improve with HBOT. Is there any support from the literature and /or would cystitis withOUT hematuria be covered by Medicare?
A: From Dr. Helen Gelly, “CMS covers both codes N30.40 and N30.41.” Please see linked excel spreadsheet for reference.
- Excel spreadsheet: Click Here
- 1
- 2